Gout is a painful form of arthritis that feels like your body is setting little fires in your joints — suddenly, intensely, and often without warning. It’s one of the most common forms of inflammatory arthritis in adults over 50, yet it remains widely misunderstood and frequently undertreated.
But what exactly is gout, what are its symptoms, and most importantly, how can you treat it?
What Causes Gout?
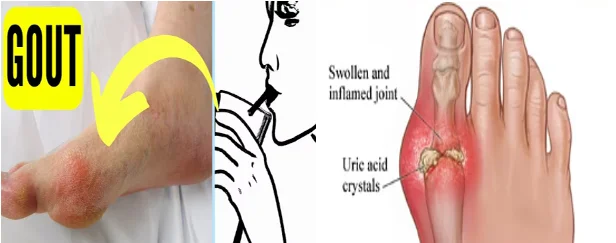
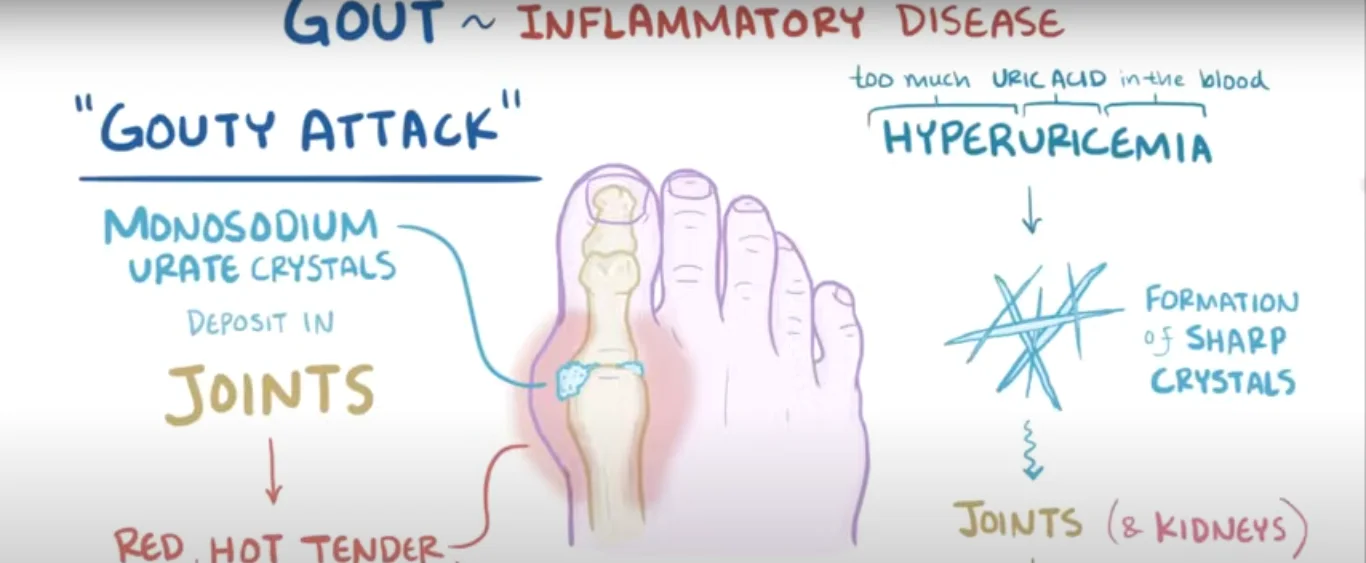
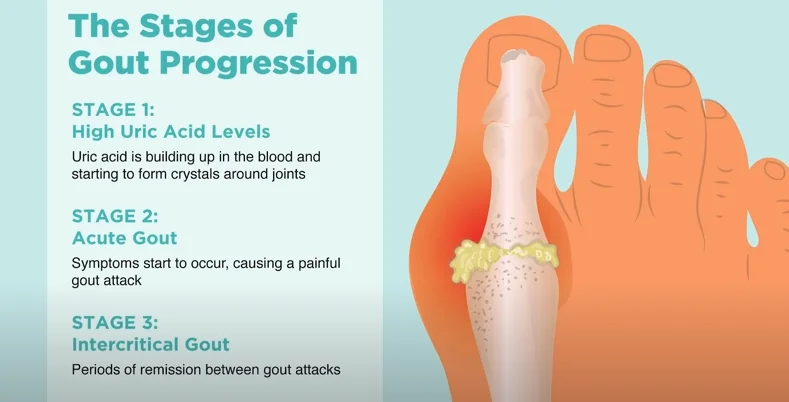
Gout is triggered when uric acid builds up in the blood and forms sharp crystals in the joints. Several factors can lead to this buildup, including a diet rich in purines (found in red meats, organ meats, and shellfish), excess alcohol consumption, obesity, and certain medications like diuretics.
Interestingly, even overweight dogs can experience joint issues from excess weight, similar to how humans develop gout-related problems — a reminder that weight management matters across species.
Uric acid is the end product of purine metabolism — a normal bodily process. In most people, uric acid dissolves in the blood, passes through the kidneys, and exits the body in urine. Gout develops when this system breaks down: either the body produces too much uric acid (overproducers, about 10% of cases), or the kidneys excrete too little of it (underexcretors, roughly 90% of cases). The result is hyperuricemia — elevated blood uric acid levels above approximately 6.8 mg/dL — at which point urate crystals begin to precipitate out of solution and deposit in cooler joint spaces.
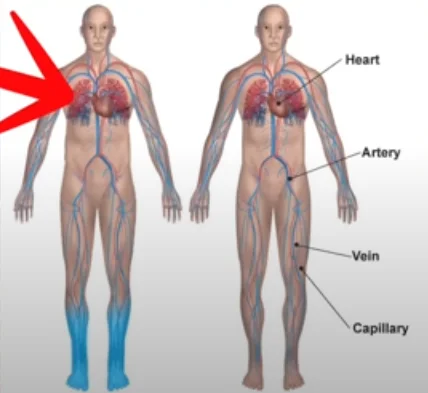
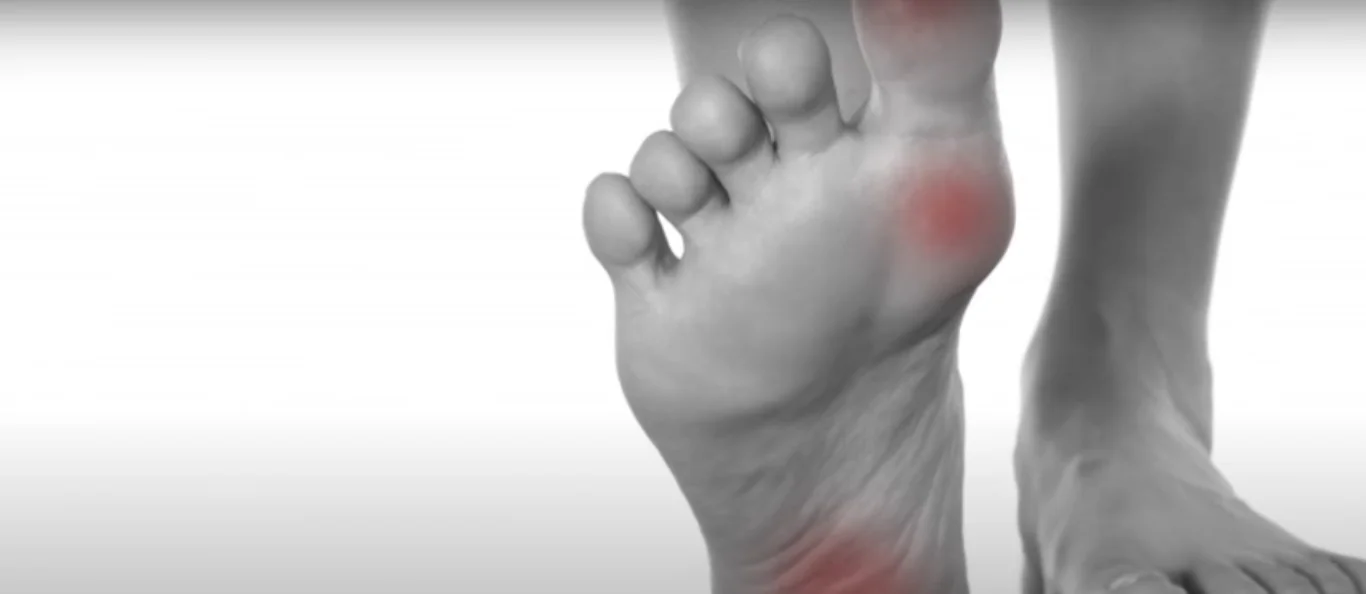
The big toe joint (first metatarsophalangeal joint) is the most common site because it’s the coolest and most distant from the heart, where urate crystals form most readily. But gout is not just a “big toe disease” — ankles, knees, wrists, and fingers are all common sites, particularly as gout progresses from intermittent to chronic. Genetics play a significant role: variants in the SLC2A9 and ABCG2 genes, which govern uric acid transport in the kidney, are strongly associated with gout risk and explain why it clusters in families.
Several medications can elevate uric acid as a side effect, most notably thiazide diuretics (commonly prescribed for blood pressure), low-dose aspirin, and cyclosporine (used in transplant patients). If you’ve recently started one of these medications and experienced a first gout attack, mention the timing to your doctor — a medication adjustment may be part of the solution.
Recognizing Gout Symptoms
Gout doesn’t always announce itself with a dramatic flare-up. Sometimes, the signs are sneakier:
- Swelling in ankles and foot inflammation
- Gout swollen foot and one ankle swollen with no pain
- Knee swelling without trauma
- Swelling around ankles and swelling on top of foot
- Finger joint swelling or swollen knuckles
- Stiff fingers in the morning or stiff back in the morning
Some people even report swollen gum around tooth, swollen belly, and systemic symptoms like stomach pain, reflecting widespread inflammation.
It’s also common to feel stiff hips, tight neck and shoulders, or a stiff lower back, sometimes confused with general aging or other arthritis types.
When gout flares badly, you might even notice swollen left foot and ankle, left ankle swelling, or swelling in only one leg — asymmetry that’s a key distinguishing feature from conditions like bilateral edema.
A classic acute gout attack is one of the most distinctive presentations in all of medicine — and if you’ve had one, you don’t forget it. The joint (most often the big toe) becomes intensely red, hot, swollen, and exquisitely tender within hours, often waking patients from sleep. The pain is frequently described as feeling like the joint is “on fire” or being “crushed.” Even the weight of a bed sheet can be unbearable. This inflammatory cascade is driven by the immune system’s response to urate crystals: white blood cells (neutrophils) engulf the crystals and release massive amounts of inflammatory cytokines — including interleukin-1β (IL-1β) — in a self-amplifying feedback loop.
Untreated, a first acute attack typically resolves on its own within 7–14 days, leading many people to dismiss it and never seek diagnosis. This is a significant missed opportunity: after a first attack, approximately 62% of patients will have a second within a year without treatment, and repeated attacks cause progressive joint damage. The intercritical period — the pain-free time between flares — shortens with each episode and eventually disappears in chronic tophaceous gout, where tophi (urate crystal deposits under the skin) become permanent fixtures.
Serum uric acid levels can actually drop during an acute attack, making blood tests taken during a flare misleadingly normal. For accurate diagnosis, ask for uric acid testing during a pain-free period, or request joint fluid analysis (arthrocentesis) during a flare — the presence of needle-shaped, negatively birefringent crystals under polarized microscopy is the gold standard for gout diagnosis.
Gout vs. Other Swelling Conditions
If you notice swelling in one foot only, right leg swelling, or lower leg swelling, it’s crucial to differentiate gout from other conditions like pseudogout (calcium pyrophosphate crystals), septic arthritis, cellulitis, or deep vein thrombosis — all of which require different treatment approaches.

Brain swelling and liver swelling are extreme inflammatory responses that show how widespread inflammation can become in severe, untreated systemic conditions.
The most important differential diagnosis for a hot, swollen joint is septic arthritis (joint infection) — a medical emergency that can destroy a joint within days if untreated. The key distinguishing factors: septic arthritis typically presents with fever, elevated white blood cell count, and a joint fluid that is cloudy with very high white cell counts (>50,000/mm³). Gout joint fluid is also inflammatory but usually lower. When in doubt — especially if there’s fever — go to urgent care or the ER rather than waiting for a scheduled appointment. The consequences of a missed joint infection are far worse than unnecessary testing.
Pseudogout (calcium pyrophosphate deposition disease, or CPPD) mimics gout closely but most commonly affects the knee rather than the big toe, tends to occur in older adults (70s–80s), and requires different long-term management. It cannot be reliably distinguished from gout without joint fluid analysis, reinforcing the value of proper diagnosis.
Deep vein thrombosis (DVT) can cause unilateral leg swelling that is sometimes confused with gout affecting the ankle or lower leg. DVT is distinguished by swelling along the path of the deep veins (rather than localized to a joint), calf tenderness, and warmth extending up the leg. DVT requires immediate anticoagulation treatment and is a medical emergency — if you’re uncertain, a doctor’s visit or urgent care evaluation is always warranted for new unilateral leg swelling.
Common Triggers That Make Gout Worse
Recommended alcohol intake is often exceeded, making flares more likely.
Swelling during pregnancy or post-pregnancy can worsen joint issues.

A very bloated stomach after heavy meals rich in purines (found in red meats, seafood, and alcohol).
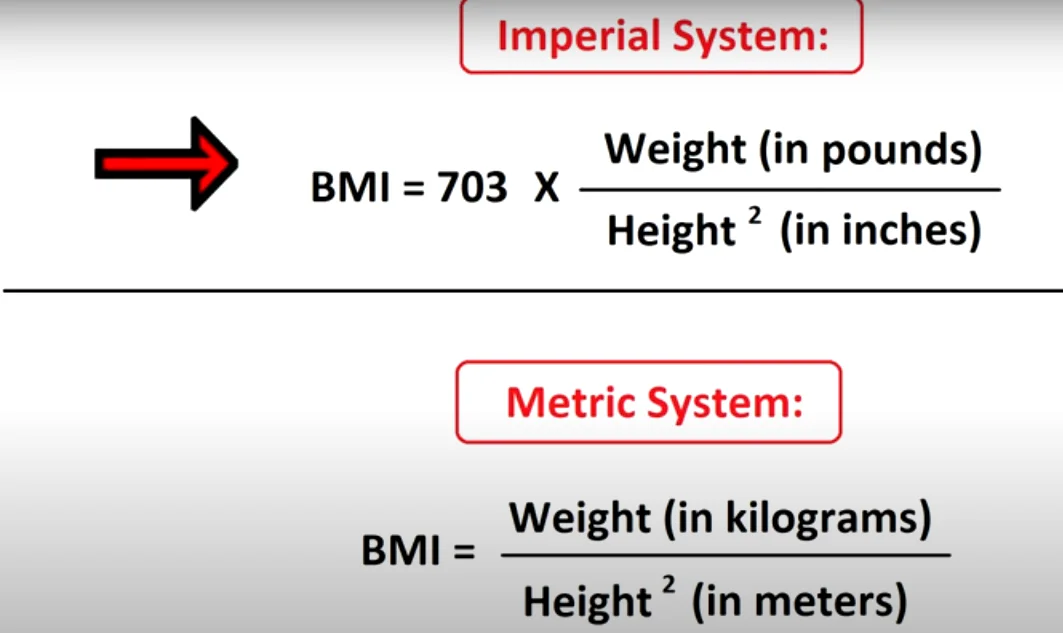
Lifestyle factors like high BMI and poor hydration.
Also note that swelling under one eye, puffy eyes, or puffy under eyes can sometimes signal kidney issues related to uric acid processing — worth mentioning to your doctor if you notice this pattern alongside joint symptoms.
Alcohol triggers gout through two separate mechanisms — making it the single most powerful dietary precipitant of flares. First, alcohol metabolism produces lactic acid, which competes with uric acid for kidney excretion, causing uric acid to accumulate in the blood. Second, beer and spirits contain purines directly. A large prospective study in The Lancet found that each additional daily alcoholic drink raised gout risk by 17%, and beer drinkers had more than double the risk of non-drinkers. Even one or two drinks in an evening can trigger a flare in someone with poorly controlled gout.
Dehydration is another major trigger that’s easy to overlook. When you’re dehydrated, uric acid becomes more concentrated in the blood and joint fluid, lowering the supersaturation threshold at which crystals form. Common dehydrating scenarios — a long flight, a hot day with inadequate water intake, a bout of diarrhea or vomiting — can reliably trigger flares in susceptible individuals. The practical rule: aim for at least 8–10 cups of fluid daily, and increase this during illness, hot weather, or alcohol consumption.
Rapid weight change — both rapid weight gain and crash dieting — can precipitate attacks. Crash dieting in particular causes cell breakdown that releases purines into the bloodstream, temporarily spiking uric acid. Sustainable, gradual weight loss (0.5–1 lb per week) through dietary changes is the safest approach for gout-prone individuals.
Effective Gout Treatments
Immediate treatments focus on reducing pain and inflammation:
Non-steroidal anti-inflammatory drugs (NSAIDs) are often the first step.
Colchicine or corticosteroids may be prescribed during acute attacks.
Lifestyle changes such as maintaining a healthy BMI help manage uric acid levels.
Long-term management involves:
- Drinking more water to prevent fluid retention in ankles.
- Reducing alcohol consumption to follow recommended daily intake.
- Managing weight through evidence-based tools.
- Considering diet changes to avoid stomach issues and purine overload.

If you suffer from stiff knees after sitting or stiff ankles, specific stretching exercises can help. Similarly, for a tight or sore neck after sleeping, targeted neck exercises can provide relief.
The cornerstone of long-term gout management is urate-lowering therapy (ULT) — most commonly allopurinol (a xanthine oxidase inhibitor that reduces uric acid production) or febuxostat. The target is a serum uric acid level below 6.0 mg/dL (or below 5.0 mg/dL in patients with tophi), at which point crystals dissolve and flare frequency drops dramatically. A critical and counterintuitive point: starting ULT can temporarily trigger a flare as crystals begin to mobilize and dissolve. This is not a treatment failure — it’s expected. Clinicians typically co-prescribe low-dose colchicine or an NSAID as “flare prophylaxis” for the first 3–6 months of ULT.
For an acute flare, timing is everything. Starting colchicine within the first 12–24 hours of symptom onset reduces the intensity and duration of the attack significantly; starting it after 48 hours provides much less benefit. Keep a small supply of your prescribed acute treatment accessible — especially when traveling — so you can begin treatment immediately rather than waiting to see a doctor.
Dietary uric acid management alone is rarely sufficient to normalize levels in established gout, but it meaningfully reduces flare frequency and medication doses required. The low-purine diet emphasizes: dairy (especially low-fat dairy, which actively lowers uric acid), complex carbohydrates, vegetables (including some high-purine ones like spinach, which are safe in gout despite their purine content), and liberal water intake. Foods to minimize: organ meats (liver, kidney), red meat in large quantities, shellfish (shrimp, crab, lobster), and all forms of alcohol.
Can Gout Affect Other Parts of the Body?
Yes! Chronic gout can lead to:
Swollen hands and feet
Swelling in underarm or swelling under chin
Swelling in toes or even swelling in wrist

Swollen gums around one tooth (similar to gum swelling causes linked with infections)
Plus, if left untreated, gout can cause kidney problems or joint deformities — not to mention worsen related inflammatory conditions.
Tophi — the chalky white deposits of urate crystals that appear under the skin in chronic gout — are a marker of severe, long-standing disease and represent a large total body urate burden. They most commonly appear on the ears, elbows, fingers, toes, and Achilles tendon. Tophi are not merely cosmetic: they cause progressive joint erosion, can ulcerate through the skin (creating infection risk), and compress surrounding tendons and nerves. The good news is that tophi are fully reversible with effective ULT maintained over 1–5 years, depending on the size of the deposits.
Kidney involvement deserves separate mention. Chronic hyperuricemia contributes to urate nephropathy and kidney stones (uric acid stones account for roughly 10% of all kidney stones in the U.S.). Men with gout have a 2–3 times higher risk of developing chronic kidney disease compared to those without gout, and kidney disease in turn impairs uric acid excretion, creating a bidirectional worsening cycle. Monitoring kidney function (creatinine, eGFR) annually is standard of care for anyone on long-term gout management.
Preventing Gout Naturally
Besides taking medications, you can help prevent flares by:
- Maintaining a healthy BMI
- Limiting alcohol intake to safe levels
- Reducing high-purine foods
- Staying active and doing gentle stretches if you’re prone to stiffness
- Managing bloating and gut inflammation to support a healthier inflammatory baseline
Cherry consumption deserves special attention as a natural gout intervention. A 2012 study in Arthritis & Rheumatism found that cherry intake was associated with a 35% lower risk of gout attacks, and cherry consumption combined with allopurinol reduced gout attack risk by 75% compared to no intervention. Cherries — particularly tart cherries — contain anthocyanins that lower uric acid levels and reduce IL-1β-driven joint inflammation. Two servings (about 10–12 cherries or 8 oz of tart cherry juice) per day during high-risk periods is a reasonable, evidence-supported natural strategy.
Vitamin C supplementation (500 mg daily) has been shown in a randomized trial published in Archives of Internal Medicine to reduce serum uric acid by approximately 0.5 mg/dL over two months — a modest but meaningful reduction that can tip borderline cases out of the crystal-formation range. Vitamin C increases renal uric acid excretion through a mechanism similar to probenecid (a uricosuric medication), making it a practical dietary adjunct.
Regular low-impact exercise — walking, swimming, cycling — helps gout prevention through two pathways: weight management (reducing the metabolic load on uric acid excretion) and improved insulin sensitivity (insulin resistance is directly associated with reduced uric acid excretion from the kidneys). Avoid high-intensity exercise during or just after a flare, as intense exertion temporarily raises uric acid through purine breakdown from muscle tissue and dehydration from sweat loss.
If you’re feeling stiff, swollen, and achy, don’t shrug it off as just getting older or a “bad night’s sleep.” Gout is highly treatable — but only if it’s properly diagnosed. Early treatment prevents joint damage, kidney complications, and the progressive shortening of pain-free intervals between flares. A simple blood test and an honest conversation with your doctor can change the trajectory of this condition entirely.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.