Inflammaging After 60: What hs-CRP and IL-6 Results Mean
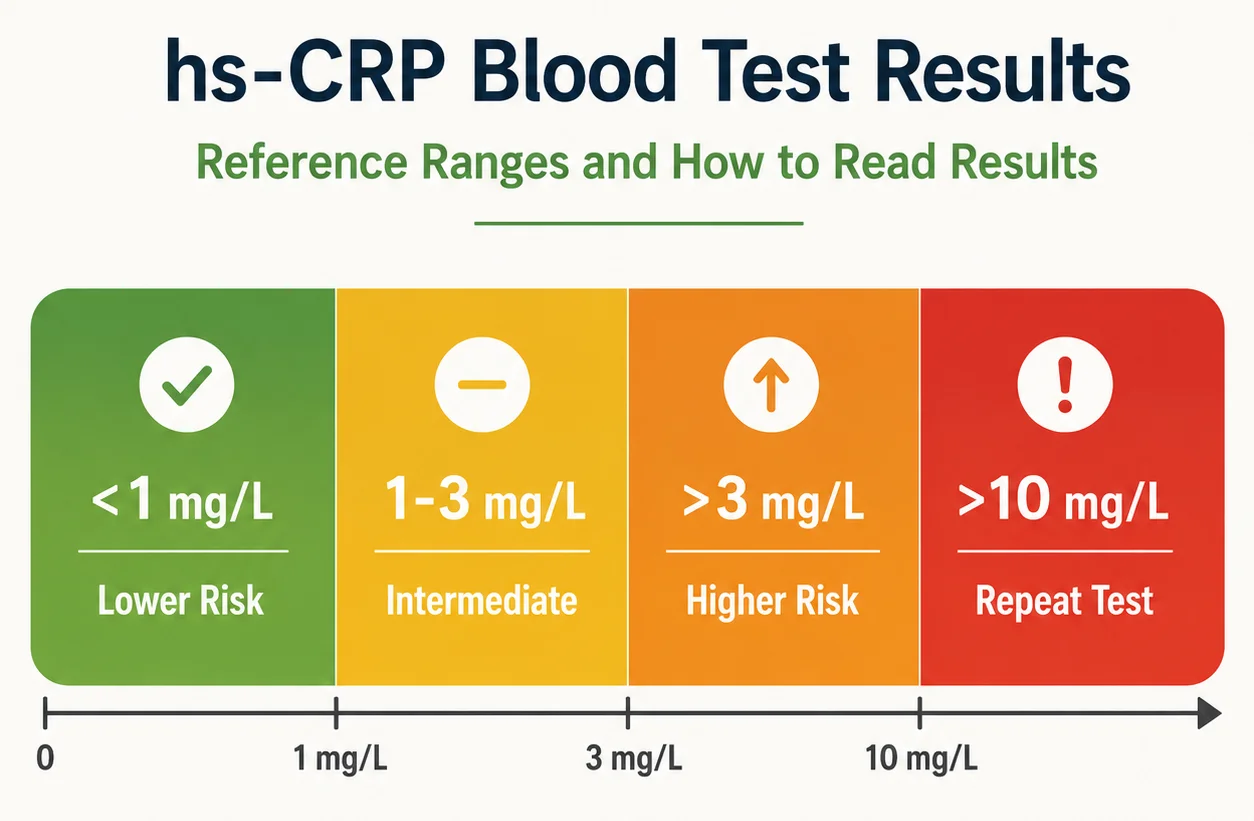
Adults over 60 with high hs-CRP or IL-6 should first rule out temporary causes such as infection, surgery, injury, or an inflammatory flare. hs-CRP is the more standardized cardiovascular marker: under 1 mg/L is lower risk, 1-3 mg/L intermediate, above 3 mg/L higher risk, and above 10 mg/L is usually repeated when you are well. IL-6 ranges vary by laboratory. Persistent elevation does not diagnose one disease; it calls for clinical review, treatment of the cause, and practical steps such as regular activity, better sleep, smoking cessation, and gradual weight management when appropriate. Seek urgent care for severe or sudden symptoms.
Executive Summary
After age 60, many people develop a background level of chronic, low-grade inflammation that researchers and the National Institute on Aging call inflammaging. It is not the same thing as a feverish infection or an autoimmune flare, but it can overlap with both. Two lab markers often discussed in this context are hs-CRP, a high-sensitivity test for very small amounts of C-reactive protein in the blood, and IL-6, an inflammatory signaling protein that sits upstream of CRP and helps drive CRP production in the liver. In older adults, both markers tend to rise on average with age, but neither test is disease-specific, and neither should be interpreted in isolation.
For most lay readers, the practical message is this: mild, persistent elevations can reflect cardiometabolic risk, excess body fat, poor sleep, smoking, frailty, arthritis, diabetes, or other chronic disease; larger spikes may suggest infection, recent injury, or another acute inflammatory process. hs-CRP has clearer cardiovascular cut points than IL-6, while IL-6 remains more assay-dependent and less standardized in routine care. Evidence-based ways to lower chronic inflammation include weight reduction when needed, regular aerobic and strength activity, better sleep, smoking cessation, and treatment of underlying conditions. Some medications help in selected settings, but they are not do-it-yourself inflammation fixes.
hs-CRP and IL-6: What Inflammaging Means After 60
The NIA defines inflammaging as age-related, chronic, sterile, low-grade inflammation that becomes more common as immune regulation changes with aging. The key word is low-grade: this is usually not the dramatic inflammation seen with pneumonia, appendicitis, or severe rheumatoid arthritis, but a quieter inflammatory “set point” that may still matter over years because it is linked to age-related disease burden.
That background inflammation matters in the United States because chronic disease is extremely common in older adults. CDC data from 2023 indicate that 93.0% of older U.S. adults reported at least one chronic condition and 78.8% reported multiple chronic conditions. That does not mean inflammaging causes every illness, but it helps explain why interpreting inflammation labs after 60 is often more complicated than simply labeling a result “normal” or “abnormal.”
How hs-CRP and IL-6 Work Together
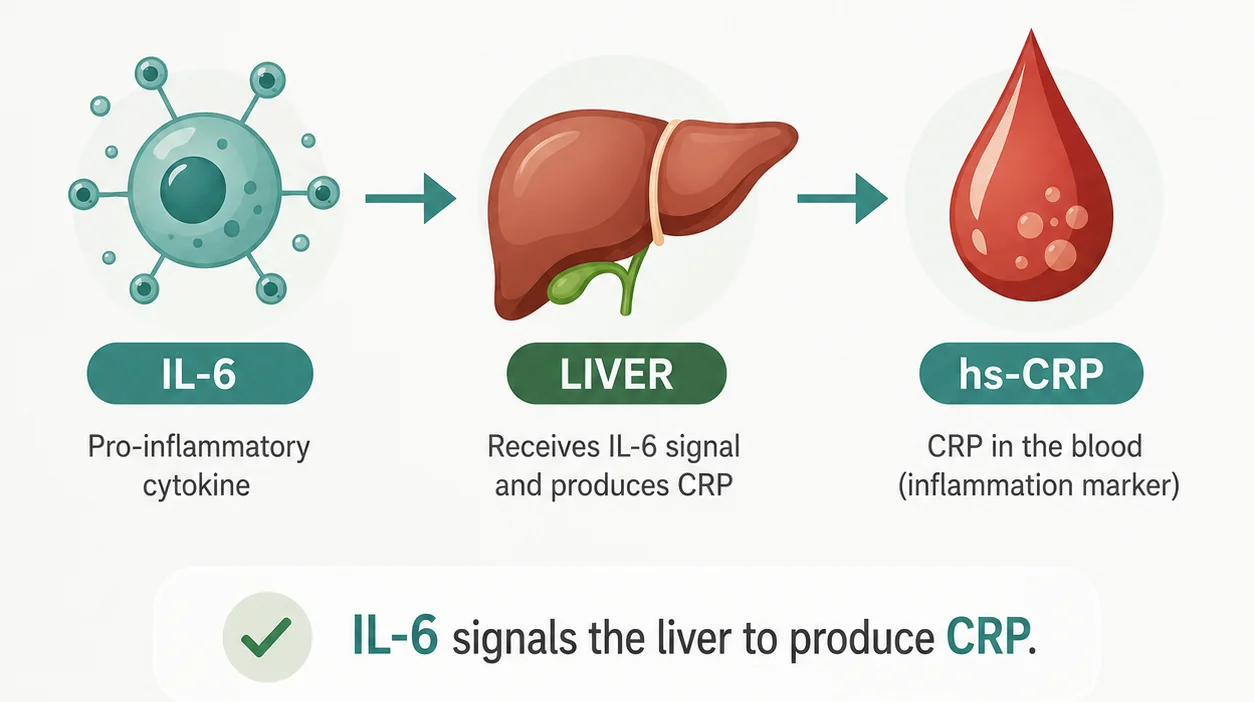
Biologically, IL-6 is a cytokine, meaning a signaling molecule used by the immune system. It helps coordinate inflammatory responses, and one of its downstream effects is to stimulate the liver to produce CRP. hs-CRP is not a different protein from CRP; it is a more sensitive way of measuring CRP at the lower concentrations relevant to cardiovascular and chronic low-grade inflammation, rather than only severe infection or tissue injury.
In plain language, IL-6 is more like an early signal, while hs-CRP is more like a downstream response marker. That is why IL-6 can be useful in research and in some specialty settings, but hs-CRP is usually easier to interpret in routine office-based cardiovascular prevention. IL-6 also has less standardized reference reporting across laboratories, which is one reason it has not become a universal screening test in primary care.
| Feature | hs-CRP | IL-6 |
|---|---|---|
| What it measures | Very low concentrations of C-reactive protein, an acute-phase protein made mainly by the liver | Interleukin-6, an upstream inflammatory cytokine |
| Typical units | mg/L | pg/mL |
| Main clinical use | Cardiovascular risk refinement; general gauge of systemic inflammation | Broader inflammatory signaling marker; more often used in specialty or research contexts |
| Strengths | Better standardized for cardiometabolic risk; widely studied in prevention | More biologically upstream; may rise earlier in inflammatory cascades |
| Limitations | Nonspecific; can rise with obesity, infection, smoking, poor sleep, and many chronic illnesses | Nonspecific; assay-dependent; less standardized reference limits and less routine primary-care use |
Sources for the comparison table: hs-CRP clinical use and interpretation come from AHA/ACC materials and reviews; IL-6 characteristics and assay limits come from Mayo Clinic Laboratories, Labcorp, and mechanistic reviews showing IL-6 drives hepatic CRP production.
Reference Ranges and How to Read Results
hs-CRP Reference Ranges After 60
For hs-CRP, the most familiar cut points are cardiovascular-risk categories rather than age-adjusted “normal ranges.” In routine preventive cardiology, values below 1 mg/L are generally considered lower risk, 1 to 3 mg/L average or intermediate risk, and above 3 mg/L higher risk. Recent ACC materials also note that hs-CRP ≥2 mg/L can act as a risk-enhancing factor when deciding whether cardiovascular prevention should be intensified. If the value is above 10 mg/L, it should usually be repeated when you are clinically stable because an acute infection or other short-term inflammatory event may be distorting the picture.
IL-6 Reference Ranges After 60
For IL-6, things are less neat. Common serum laboratory reference limits in U.S. labs are often around less than 6.4 pg/mL or less than 7 pg/mL, but those limits vary by assay platform and laboratory method. A meta-analysis of healthy individuals estimated a pooled IL-6 value of about 5.19 pg/mL and found that IL-6 rose by roughly 0.05 pg/mL per year of age, reinforcing that age shifts baseline levels upward on average. Still, there is no widely adopted clinical age-adjusted IL-6 range used across U.S. routine practice, so the safest approach is to interpret IL-6 against the reporting laboratory’s own reference interval and the clinical context.
That same caution applies, though to a lesser degree, to hs-CRP. Older age, female sex, obesity, smoking, insomnia, depression, and hormone therapy can all push CRP upward even without a new disease being discovered on that day. In other words, a “high” hs-CRP often reflects a burden of risk and physiology, not a diagnosis by itself.
| Marker | Common Adult Reference Approach | Age-Adjusted Range in Routine U.S. Practice | What a Mildly High Result Often Means |
|---|---|---|---|
| hs-CRP | <1 mg/L lower CV risk; 1–3 mg/L average; >3 mg/L higher risk; >10 mg/L usually repeat when well | Not routinely used; fixed cardiometabolic thresholds are more common | Residual inflammatory risk, obesity, smoking, sleep problems, chronic disease, or subclinical cardiometabolic stress |
| IL-6 | Often lab-specific upper limit around <6.4 to <7 pg/mL | Not standardized; aging raises averages, but universal age-adjusted cut points are not established | General inflammatory activation; may reflect infection, chronic inflammatory disease, frailty, or cardiometabolic burden |
Interpretation note: these are practical clinical-use ranges, not guarantees of health or disease, and they assume standard serum assays rather than research-only testing platforms.
Why Repeat Testing Matters
One older but still useful AHA/CDC principle is that hs-CRP is more stable if measured at least twice and averaged, ideally a couple of weeks apart when there is no acute illness. That is especially important when the decision in front of you is not “Do I have inflammation?” but rather “Does this result meaningfully change my cardiovascular risk management?”
A final practical assumption belongs here: unless the lab report specifies otherwise, this article assumes your hs-CRP is being interpreted in mg/L and your IL-6 in pg/mL. If a standard CRP test is reported in mg/dL, that is a different reporting convention and should not be read using hs-CRP cardiovascular cut points.
What High Results Can Mean for Health After 60
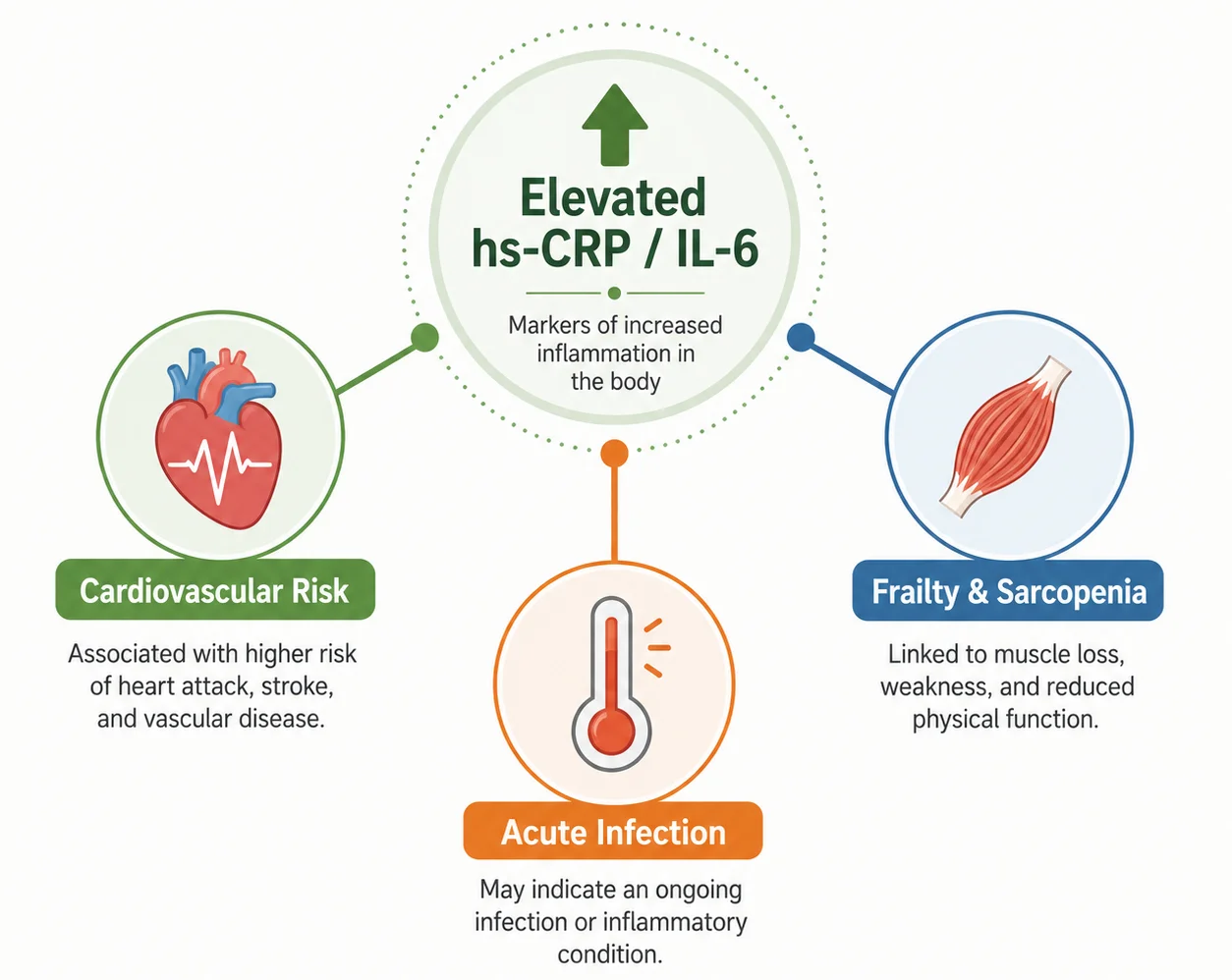
Cardiovascular Risk and Residual Inflammation
A persistently modestly elevated hs-CRP often functions as a sign of residual inflammatory risk, especially for cardiovascular disease. ACC/AHA prevention guidance and later cardiology statements support using hs-CRP as one of the tools that can refine risk when the treatment decision is uncertain. In this setting, the result does not diagnose blocked arteries by itself, but it can help identify people who may benefit from more aggressive lifestyle work and, in some cases, statin therapy or other risk-lowering treatment.
That cardiovascular link is not theoretical. In the JUPITER trial, apparently healthy adults with LDL cholesterol below 130 mg/dL but hs-CRP at or above 2 mg/L experienced fewer major vascular events when treated with rosuvastatin, and the drug lowered both LDL cholesterol and hs-CRP. This does not mean everyone with a high hs-CRP should take a statin, especially after age 75, when shared decision-making becomes more individualized, but it does show that elevated hs-CRP sometimes flags a preventable risk state rather than a meaningless number.
Frailty, Sarcopenia and Mobility
Frailty and mobility decline are another important part of the story after 60. Systematic reviews and cohort studies show that IL-6 and CRP are repeatedly associated with frailty, weaker muscle performance, poorer walking speed, and sarcopenia in older adults. This is one reason these markers attract geroscience interest: they may not simply reflect disease, but also the loss of physiologic reserve that makes a person more vulnerable to falls, disability, and stressors.
Acute Infection and Other Inflammatory Causes
When the numbers are much higher, the interpretation changes. A very high CRP or rapidly rising IL-6 is more suggestive of an acute inflammatory event than of background inflammaging. Infections, inflammatory bowel disease, autoimmune flares, tissue injury, and other acute illnesses can all raise CRP. MedlinePlus and lab references specifically warn that CRP is nonspecific and that IL-6 elevations can also occur with systemic or localized infection and chronic inflammatory disease.
This is why labs must be interpreted alongside symptoms. If you have fever, chills, new cough, shortness of breath, painful urination, sudden joint swelling, severe dental symptoms, or a recent surgery or injury, the result may be telling your clinician something very different from “age-related chronic inflammation.” A number that suggests vascular risk in a well person may signal infection in a sick person.
Finally, high hs-CRP and IL-6 can accompany many chronic conditions common after 60, including obesity, diabetes, smoking-related disease, autoimmune disorders, chronic lung disease, inflammatory bowel disease, and some cancers. That is why persistent elevation should prompt a search for causes, not reflexive supplement shopping.
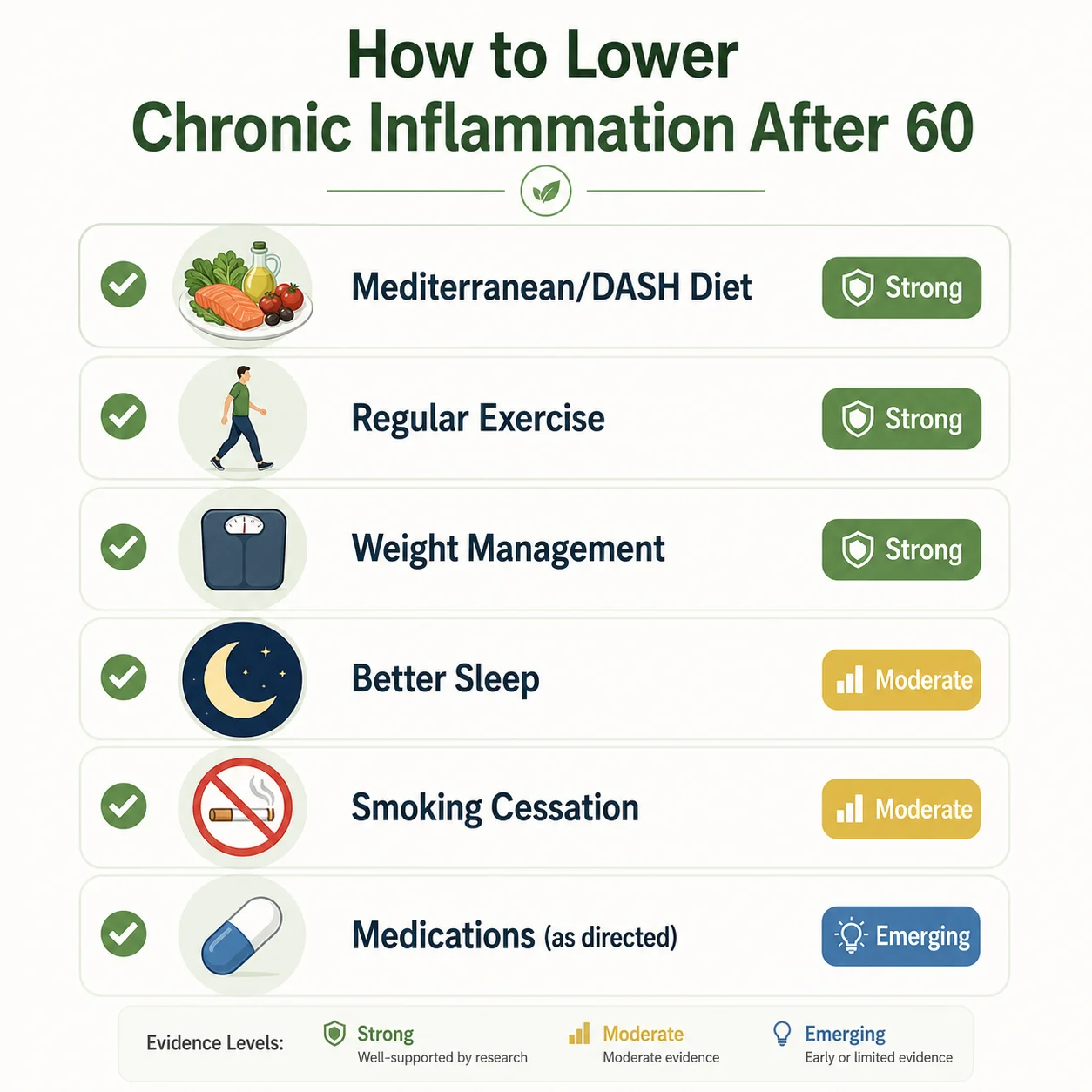
How to Lower Chronic Inflammation After 60
The most evidence-based way to lower chronic inflammation is usually not a single anti-inflammatory product. It is a package: address excess visceral and total body fat if present, move regularly, sleep adequately, stop smoking, improve diet quality, and treat the chronic diseases that are actually driving the inflammation. These interventions are also consistent with U.S. preventive guidance from HHS, CDC, AHA, and USPSTF.
Mediterranean-Style and DASH Eating Patterns
Diet quality matters, but older adults should not expect a miracle from one “anti-inflammatory food.” The best-supported patterns are Mediterranean-style and DASH-style eating, emphasizing vegetables, fruit, legumes, whole grains, unsaturated fats such as olive oil, and healthy protein sources. AHA materials summarize evidence that these patterns can lower hs-CRP, and controlled feeding research has found beneficial effects on inflammatory and cardiovascular biomarkers, although not every diet trial shows identical CRP changes. The bigger lesson is that diet works best as a pattern, especially when it helps with weight control and blood pressure. For meal ideas built around this pattern, see our list of 10 best foods to eat every day after 60.
Aerobic, Strength and Balance Exercise
Exercise is one of the most practical anti-inflammatory tools because it helps at several levels at once: body composition, insulin sensitivity, blood pressure, mood, function, and inflammation. U.S. guidance for older adults recommends at least 150 minutes of moderate-intensity aerobic activity each week, muscle-strengthening activity at least 2 days per week, and balance work. Trials and reviews in older adults suggest that exercise can lower CRP more consistently than IL-6, while structured resistance training and combined lifestyle programs can improve function and reduce inflammatory markers in many participants. For a structured starting routine, see our guide to building muscle after 60 with cheap everyday foods.
Weight Management Without Losing Muscle
Weight loss, when clinically appropriate, may be the single most powerful lifestyle lever for many people with elevated inflammatory markers after 60 because adipose tissue itself contributes to inflammatory signaling. Randomized studies in older adults show that intentional weight reduction can reduce both CRP and IL-6, and achieving around 5% weight loss is associated with substantially better odds of reaching more desirable inflammatory levels. This is especially relevant if high hs-CRP travels with central obesity, insulin resistance, fatty liver, or osteoarthritis.
Sleep Quality and Sleep-Apnea Evaluation
Sleep is often an underappreciated driver. AHA materials now include sleep as part of overall cardiovascular health, and poor sleep quality or insomnia is linked to inflammatory signaling. This does not mean one bad night will “cause inflammaging,” but chronic sleep disruption, untreated sleep apnea, and inconsistent sleep can keep inflammation higher over time. For most adults, the broad AHA target remains 7 to 9 hours of sleep per night. If CPAP-related sleep issues are part of the picture, see our guide on CPAP dry mouth in older adults.
Smoking Cessation
Smoking cessation also belongs near the top of the list. Smoking can raise CRP, and studies suggest that quitting has a favorable long-term effect on inflammatory burden, even if improvement is not immediate. For older adults, this is a major opportunity because the same step that lowers inflammatory tone also lowers cancer, COPD, vascular, and stroke risk.
Prescription Treatment When Clinically Indicated
For medications, the strongest general message is: treat the underlying condition, not just the biomarker. Statins can lower hs-CRP and reduce cardiovascular events in appropriate patients; the evidence is strong in primary prevention for selected adults and in secondary prevention more broadly. After age 75, prevention decisions become more individualized, but hs-CRP can still help frame the discussion.
Low-dose colchicine is different. It has randomized-trial evidence for reducing cardiovascular events in some people with established chronic coronary disease, but it is not a general-purpose treatment for age-related inflammation. It can cause gastrointestinal side effects, it interacts with other drugs, and kidney or liver disease can complicate its use. In other words, colchicine is a cardiology drug for selected patients, not a self-directed hs-CRP fixer.
Supplements: Evidence, Limits and Safety
As for supplements, the evidence is weaker and more mixed than marketing suggests. Omega-3 fatty acids have moderate evidence for small improvements in CRP and IL-6 in meta-analyses, but they should not replace diet quality or evidence-based cardiovascular care. Higher doses can interact with medications and may increase bleeding concerns in some settings, even though major bleeding effects are not consistently seen in studies. Curcumin has low-to-moderate evidence for lowering CRP and IL-6 in meta-analyses, but product quality varies and drug interaction issues remain real. Vitamin D should primarily be used to correct deficiency and support bone health rather than as a standalone inflammation treatment; meta-analyses on inflammatory biomarkers are mixed, and excessive supplementation can cause hypercalcemia and kidney complications.
| Strategy | Evidence Level | What the Evidence Supports | Key Cautions |
|---|---|---|---|
| Mediterranean or DASH-style eating | Moderate to high | Can improve cardiometabolic health and may lower hs-CRP | Effect size varies; pattern matters more than one “superfood” |
| Regular aerobic exercise | High | Lowers hs-CRP modestly and improves overall health | Start gradually if deconditioned |
| Strength training | Moderate | Improves function; some studies show lower IL-6 | Needs safe progression, especially with arthritis or frailty |
| Intentional weight loss if overweight or obese | High | Often lowers CRP and IL-6 more than exercise alone | Avoid crash dieting; preserve muscle with protein and resistance work |
| Better sleep and sleep-disorder treatment | Moderate | Linked to lower inflammatory burden and better heart health | Evaluate sleep apnea if snoring/daytime sleepiness are present |
| Smoking cessation | High | Lowers inflammatory burden over time and strongly improves overall risk | Benefits increase with sustained abstinence |
| Statins when otherwise indicated | High | Lower LDL and hs-CRP; reduce events in selected patients | Prescription treatment; decision is individualized, especially after 75 |
| Colchicine for established coronary disease | Moderate to high in selected patients | Lowers events in some secondary-prevention patients | GI side effects; drug interactions; kidney/liver cautions |
| Omega-3 supplements | Moderate for biomarkers, lower for outcome targeting of “inflammaging” itself | Small biomarker improvements are possible | Medication interactions; do not use as sole therapy |
| Curcumin | Low to moderate | Some biomarker reduction in meta-analyses | Product quality and interactions vary |
| Vitamin D | Mixed | Use mainly for deficiency, not simply high hs-CRP or IL-6 | Excess can cause hypercalcemia and kidney injury |
Evidence-level note: these labels are editorial shorthand for readers, not formal USPSTF or GRADE ratings. Supporting sources are cited in the paragraph above.
What To Do After a High Result
First Check for Temporary Causes
If your result is high, the first step is not panic. The key questions are whether you were well when the blood was drawn, whether the elevation is mild or large, and whether there are other clues such as fever, new symptoms, recent surgery, dental infection, worsening arthritis, or changes in weight, blood sugar, or blood pressure. hs-CRP values above 10 mg/L generally deserve repeat testing when you are stable because short-term illness can temporarily dominate the result.
Review the Full Cardiometabolic and Functional Picture
The next practical step is to ask whether the test changes management. For hs-CRP, that may mean reviewing cholesterol, blood pressure, smoking, diabetes risk, obesity, sleep, and exercise. For IL-6, it may mean asking why the test was ordered in the first place, because IL-6 is more often used when a clinician is evaluating broader inflammatory or specialty questions. Persistent elevation in either marker should trigger a thoughtful search for contributors, not a reflex conclusion that “this is just aging.”
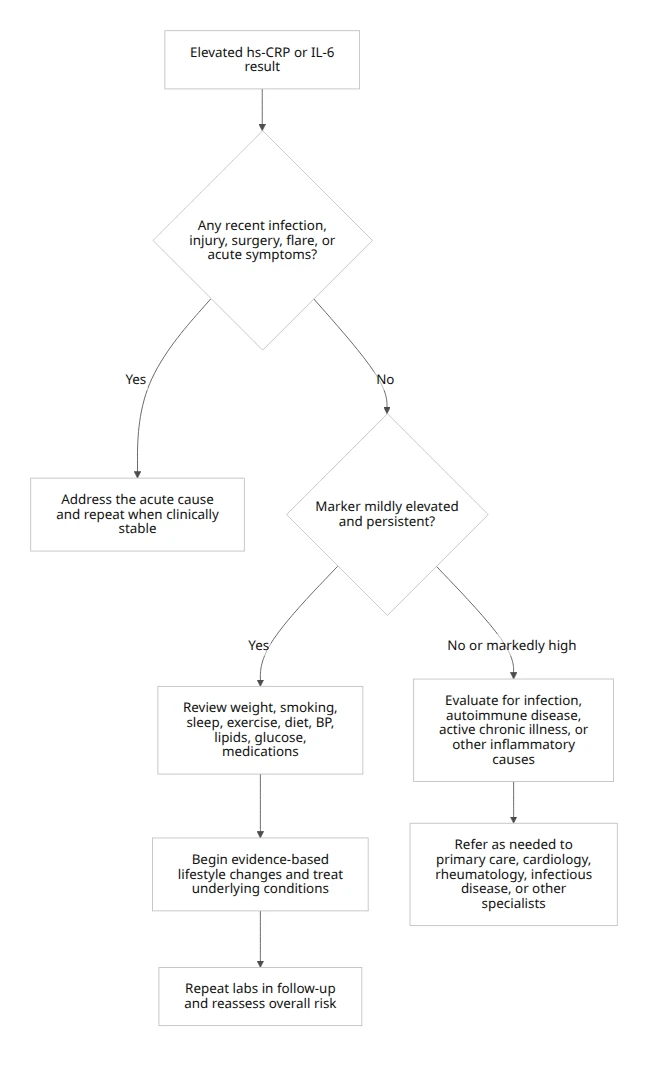
This flow is based on AHA/ACC guidance for hs-CRP interpretation, the recommendation to repeat hs-CRP when it is above 10 mg/L and the patient is stable, and general NIH/MedlinePlus cautions that CRP and IL-6 are nonspecific markers whose meaning depends on symptoms and clinical context.
For many adults over 60, a sensible real-world follow-up visit includes a medication review, blood-pressure check, lipid discussion, diabetes screening if indicated, smoking review, weight and waist discussion, sleep assessment, and functional questions such as gait, falls, strength, and fatigue. That approach reflects the fact that elevated inflammatory markers can point both to cardiovascular risk and to aging-related vulnerability, especially frailty.
FAQs
No. Inflammaging is not an official disease diagnosis. It is a scientific and clinical concept describing chronic, sterile, low-grade inflammation that becomes more common as immune regulation changes with age and is associated with several age-related conditions.
Yes. hs-CRP and standard CRP measure the same C-reactive protein. The difference is sensitivity: hs-CRP detects lower baseline concentrations used for cardiovascular-risk refinement and chronic low-grade inflammation, while standard CRP is commonly used for larger inflammatory responses.
Above 3 mg/L is generally considered higher cardiovascular risk when hs-CRP is measured in a clinically stable person. Values below 1 mg/L are lower risk, 1-3 mg/L intermediate, and 2 mg/L or higher may count as a risk-enhancing factor in some prevention decisions.
Above 10 mg/L is generally too high to interpret as stable low-grade cardiovascular inflammation without reassessment. The test is usually repeated after an infection, injury, surgery, or inflammatory flare has resolved because acute illness can temporarily dominate the result.
No universal age-adjusted normal IL-6 range exists for older adults. Many U.S. laboratories use assay-specific upper limits near 6.4-7 pg/mL, but the reporting laboratory’s own reference interval, symptoms, and other test results should guide interpretation.
Yes. IL-6 tends to rise gradually with age on average, but age alone does not explain every elevation. A high result still needs to be interpreted in relation to the laboratory method, current symptoms, medications, body composition, and chronic conditions.
Yes. Excess adipose tissue, particularly visceral fat, can produce inflammatory signals and is associated with higher hs-CRP and IL-6. When weight loss is medically appropriate, gradual loss combined with adequate protein and resistance exercise may lower inflammation while helping preserve muscle.
Yes. Persistent poor sleep, insomnia, irregular sleep, and untreated sleep apnea are associated with inflammatory signaling. One bad night does not diagnose inflammaging, but ongoing sleep problems should be addressed as part of cardiovascular and metabolic risk management.
No. High hs-CRP or IL-6 does not automatically mean infection. Mild persistent elevations may reflect chronic cardiometabolic or inflammatory burden, whereas larger or rapidly rising values are more concerning when accompanied by fever, cough, urinary symptoms, pain, swelling, or recent injury.
Yes. Higher IL-6 and CRP levels are associated with frailty, slower walking, weaker muscle performance, and sarcopenia in older adults. The markers do not diagnose frailty by themselves, so function, strength, falls, weight change, and mobility still require direct assessment.
No. Routine IL-6 screening is not recommended for every adult over 60. The test is less standardized than hs-CRP and is usually ordered for a specific clinical, specialty, or research reason rather than as a general wellness screen.
No. A high hs-CRP result alone is not a reason for everyone to start a statin. Treatment depends on the complete cardiovascular-risk profile, including age, LDL cholesterol, blood pressure, diabetes, smoking, established vascular disease, medication tolerance, and patient preference.
No. Exercise does not usually lower inflammation overnight. Consistent aerobic and resistance activity may reduce hs-CRP over time while also improving blood pressure, glucose control, body composition, strength, balance, and function.
No. Supplements alone are not enough to correct persistently high inflammation markers. Omega-3 or curcumin may produce modest biomarker changes in some studies, but they do not replace evaluation of the cause, exercise, sleep, smoking cessation, weight management, or prescribed treatment.
No. Do not start aspirin or ibuprofen solely to lower hs-CRP or IL-6 without medical advice. Starting aspirin for primary prevention is generally discouraged in adults 60 or older, and NSAIDs can increase bleeding, kidney, blood-pressure, and gastrointestinal risks.
Authoritative Outbound Sources Used
The following official and clinically authoritative sources support the medical, laboratory, cardiovascular, exercise, sleep, nutrition, and safety guidance used in this article.
- National Institute on Aging – Inflammaging Workshop
- MedlinePlus – C-Reactive Protein Test
- Mayo Clinic Laboratories – Interleukin-6 Test
- American Heart Association – hsCRP Toolkit
- CDC – Multiple Chronic Conditions in Older Adults
- CDC – Physical Activity for Older Adults
- New England Journal of Medicine – JUPITER Trial
- New England Journal of Medicine – Colchicine in Chronic Coronary Disease
- American Heart Association – Sleep and Cardiometabolic Health
- USPSTF – Aspirin for Cardiovascular Prevention
Medical note: These resources are provided for education and further reading. Personal test interpretation, medication, supplement, nutrition, and exercise decisions should be reviewed with a qualified healthcare professional.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.