

Nootropics After 60: What Really Works?
Most nootropic supplements and memory pills do not reliably improve cognitive function or prevent dementia in adults over 60. Morning caffeine can temporarily sharpen alertness, and plain creatine monohydrate has limited evidence for selected short-term memory tasks. Trendy options such as mushroom coffee remain clinically unproven. Before starting a cognitive booster, ask a clinician or pharmacist to review prescription interactions, kidney function, and treatable causes of brain fog.
Evidence context: National Institute on Aging and FDA dietary-supplement guidance
Explore related guidance in KeepFitQuote’s Brain & Mental Health hub.
Try This 60-Second Brain-Fog Safety Check
Choose the line that best matches your situation. This check is not a diagnosis; it helps you decide whether shopping for a supplement is appropriate today. The CDC’s stroke warning signs emphasize sudden neurological changes because treatment is time-sensitive.
Sudden facial droop, one-sided weakness, speech trouble, severe new headache, loss of balance, collapse, seizure, chest pain, or inability to stay awake: call 911.
New confusion over hours or days, especially after a medication change, infection, fall, dehydration, or low blood sugar: contact a clinician promptly.
Gradual memory change that affects driving, medicines, bills, cooking, or navigation: arrange a medical assessment rather than testing a “memory booster.”
Stable, mild mental fatigue without red flags: review sleep, medicines, mood, hearing, diet, alcohol, activity, and medical conditions before considering one controlled experiment.
Interactive pause: write down when the problem began, whether it fluctuates, and one real task it affects. “My brain feels off” is difficult to measure. “I reread the same paragraph four times after lunch” is specific enough to investigate and track.
What Counts as a Nootropic After 60?
“Nootropic” is a marketing and umbrella term, not an FDA-approved treatment category. The FDA’s dietary-supplement overview explains how supplements are regulated in the United States. The nootropic label may refer to caffeine, vitamins, amino acids, herbs, mushroom extracts, creatine, omega-3 fats, multi-ingredient powders, or non-pill approaches such as cognitive training, meditation, exercise, and sleep improvement.
These interventions are not interchangeable. A stimulant may temporarily increase alertness without improving memory storage. A vitamin can correct a deficiency but do nothing when levels are adequate. A training game may improve the task being practiced without helping medication management or driving. A product may influence a laboratory marker without changing a meaningful daily outcome.
For adults over 60, the useful question is not “Is this a nootropic?” It is: What outcome was tested, in whom, for how long, against what comparison, and with what risks? KeepFitQuote’s guide to how brain dopamine shapes motivation, attention, and behavior illustrates why a real neurotransmitter mechanism does not automatically validate a “dopamine-boosting” product. The label “natural” does not answer any of those questions.
How U.S. Regulatory Categories Differ
| Category | Meaning in the USA |
|---|---|
| Prescription medicine | FDA-approved for a defined indication after review of evidence; it should not be treated as a synonym for any product marketed as a nootropic. |
| Dietary supplement | Regulated as a food category and not FDA-approved for effectiveness before sale; manufacturers are responsible for lawful labeling and product safety. |
| Botanical extract | Usually sold as a dietary supplement. Evidence applies only to the exact species, plant or fungal part, preparation, standardization, amount, and population studied. |
| Experimental compound | An unapproved or research-stage substance that is not appropriate for routine self-treatment, especially when identity, purity, interactions, and human safety are uncertain. |
| Cognitive training | A non-drug intervention. Evidence is normally task-specific; improvement on a trained skill does not automatically prove broad memory improvement or dementia prevention. |
Source: FDA 101: Dietary Supplements.
Why Brain Fog Needs a Cause Before a Supplement
Brain fog can mean slow recall, poor concentration, word-finding difficulty, sleepiness, reduced mental stamina, or feeling detached. Causes include fragmented sleep, sleep apnea, depression, anxiety, pain, hearing loss, thyroid disease, anemia, vitamin B12 deficiency, diabetes, infection, dehydration, alcohol, and medication effects. The National Institute on Aging’s cognitive-health guidance places medical conditions, medicines, sensory health, sleep, and lifestyle in the same decision framework.
A supplement-first approach can mask the timeline and delay treatment. Diphenhydramine, some bladder medicines, benzodiazepines, opioids, sleep drugs, and anticholinergic combinations may impair attention or memory. Untreated hearing loss can look like forgetting because information was never heard clearly. KeepFitQuote’s Internal Terrain After 60 framework for medicines, nutrition, sleep, movement, stress, and hydration helps readers examine connected causes without reducing symptoms to one supplement target.
Solution prompt: list three changes from the month before symptoms began—new medicine, illness, grief, travel, sleep disruption, alcohol, diet, pain, or reduced activity. KeepFitQuote’s guide to an elderly parent who is sleepy and confused explains why quiet delirium can be mistaken for ordinary tiredness or aging. Bring the timeline to a clinician; finding and treating the driver is more powerful than adding an unproven blend.
What Really Works: An Evidence Ladder
Use an evidence ladder. The National Center for Complementary and Integrative Health explains how to judge health research before applying a claim to yourself. At the top are interventions with repeated randomized trials, meaningful outcomes, acceptable safety, and relevance to people like you. In the middle are plausible interventions with small or inconsistent trials. At the bottom are testimonials, animal studies, and before-and-after stories without a comparison group.
Best-supported foundations: regular aerobic and resistance activity, adequate sleep, treatment of sleep apnea, blood-pressure and diabetes management, hearing correction when needed, social and intellectual engagement, and correction of documented deficiencies.
Situation-dependent tools: caffeine for alertness, creatine for selected memory or fatigue outcomes, and structured cognitive training for practiced abilities.
Uncertain products: mushroom coffee, lion’s mane extracts, bacopa, multi-herb blends, and many branded “neuro” formulas.
Poor bets: proprietary blends with hidden amounts, products claiming to reverse dementia, and stacks containing multiple stimulants or drug-like ingredients.
Evidence is not a popularity contest. A product can have thousands of reviews and still lack a blinded trial. Conversely, a small measurable benefit may be worthwhile when the intervention is safe, inexpensive, and linked to a goal you value.

Evidence Matrix: Nootropic Options After 60
| Option | Evidence Grade | Possible Outcome | Main Limitation or Risk |
|---|---|---|---|
| Lifestyle foundations | Strongest practical support | Brain and cardiovascular health, function | Requires sustained habits; not an instant treatment |
| Caffeine | Established for short-term alertness | Wakefulness and reaction time | Sleep disruption, anxiety, palpitations, blood pressure |
| Creatine monohydrate | Promising but limited for cognition | Selected memory, attention, or fatigue tasks | Mixed results; kidney-test interpretation and fluid context |
| Cognitive training | Moderate for trained abilities | Practice-specific speed, recall, or reasoning | Transfer to everyday cognition is uncertain |
| Vitamin replacement | Strong only for documented need | Correction of deficiency-related symptoms | Little reason for high doses when status is adequate |
| Lion’s mane / mushroom coffee | Emerging or insufficient | Uncertain memory or mental-fatigue effects | Product variability, small studies, interactions |
| Ginkgo and multi-herb blends | Mixed or unsupported for prevention | No reliable dementia-prevention benefit | Bleeding and medicine interactions; hidden amounts |
Ingredient-Specific Evidence Details
| Option | Population, Form, and Duration Studied | Outcome and Evidence Grade | Common Adverse Effects or Major Concerns |
|---|---|---|---|
| Lifestyle foundations | Not one product trial: evidence spans older-adult physical activity, vascular-risk control, sleep, hearing, and engagement; benefits require sustained practice. | Brain, cardiovascular, and daily-function support; strongest practical foundation, but no single habit prevents dementia. | Exercise and diet changes must match frailty, falls, heart, kidney, diabetes, and medication considerations. |
| Caffeine | Acute caffeine exposure in coffee, tea, or measured products; no single defining trial establishes a universal regimen for adults over 60. | Alertness and reaction-time effects are established; evidence does not show treatment of the cause of brain fog. | Insomnia, anxiety, tremor, reflux, urinary urgency, palpitations, and blood-pressure effects; total caffeine from all sources matters. |
| Creatine monohydrate | Sixteen RCTs; 492 adults aged 20.8–76.4; three studies specifically enrolled adults 60+; interventions were shorter or longer than four weeks. | Signals for memory, attention time, and processing speed; no significant overall cognitive or executive-function benefit. Moderate certainty for memory; low for several other outcomes. | GI upset and water-weight change may occur. Kidney disease, fluid restrictions, heart failure, and interpretation of creatinine tests require clinician review. |
| Cognitive training | ACTIVE: 2,832 independent older adults, mean age 73.6; ten memory, reasoning, or speed sessions over five to six weeks, with some booster sessions. | Improved trained abilities; reasoning and speed effects persisted in follow-up. Broad transfer is limited and dementia prevention is not established. | Frustration, fatigue, cost, accessibility, and lost sleep can outweigh benefit; training should resemble the real-life skill being targeted. |
| Vitamin B12 replacement | People with clinically confirmed deficiency; exact oral or injectable form and duration depend on cause, absorption, symptoms, and laboratory findings. | Strong for correcting a documented deficiency; not a general cognitive enhancer when B12 status is adequate. | Diagnosis may require B12 plus confirmatory markers; kidney function can affect methylmalonic acid interpretation. Treatment should address the underlying cause. |
| Lion’s mane | One small trial randomized 30 Japanese adults aged 50–80 with mild cognitive impairment to a defined 96% dry-powder tablet preparation or placebo for 16 weeks. | Cognitive-scale scores improved during treatment but fell after stopping; emerging, very-low-certainty evidence that cannot validate mushroom coffee or unrelated extracts. | Exact species, fungal part, extraction, contaminants, allergy risk, GI symptoms, glucose or bleeding concerns, and medication interactions require review. |
| Ginkgo | GEM trial: more than 3,000 adults age 75+ with normal cognition or mild cognitive impairment; standardized extract versus placebo for a median of six years. | No reduction in dementia or Alzheimer’s disease incidence; unsupported for prevention and inconsistent for cognitive symptoms. | Dizziness, GI symptoms, headache, and bleeding risk, particularly with anticoagulant or antiplatelet therapy; other drug interactions are possible. |
Evidence-use note: These study details describe the tested populations and preparations; they are not a universal dosing protocol. Adults over 60 should have medicines, kidney and liver status, cardiovascular risks, and the intended outcome reviewed before beginning a supplement.
How to Read a Nootropic Study Without Being Misled
First, check the population. The National Library of Medicine’s clinical-research guide distinguishes human clinical studies from earlier research. A laboratory experiment, mouse study, or trial in sleep-deprived college students does not establish benefit for a 70-year-old managing hypertension and several medicines. Look for participants’ ages, diagnoses, baseline cognition, medication use, and the number who completed the study.
Second, inspect the intervention. The exact extract, chemical form, amount, schedule, and duration matter. A standardized lion’s mane extract cannot validate an unspecified mushroom powder. A creatine-monohydrate trial cannot prove that a branded “brain creatine” blend is better. If the commercial label hides ingredient amounts, the research cannot be matched to the product. Also check whether the comparison group received a convincing placebo and whether participants and researchers were blinded.
Third, identify the outcome. Statistical improvement on one computerized task may be real but too small to notice in daily life. A study that tests 20 outcomes may find one positive result by chance, especially when it was not selected in advance. Favor studies that define a primary outcome, report absolute changes, describe adverse events, and measure function such as medication accuracy, independent living, or sustained task performance—not only a laboratory score.
Fourth, separate association from causation. People who drink tea, exercise, or use supplements may also have different diets, income, education, healthcare access, or social activity. An observational association cannot prove the product caused the outcome. Random assignment reduces this problem, while systematic reviews can show whether results repeat across studies. Reviews are still only as strong as the trials they include, so “meta-analysis” is not an automatic guarantee.
Finally, look for replication and conflicts. One positive study funded by a manufacturer is a starting point, not a conclusion. Funding does not automatically invalidate research, but methods, registration, missing data, selective reporting, and author relationships deserve scrutiny. Ask whether an independent group reproduced the finding with the same product and whether benefits persisted after treatment. If the only available evidence appears on a seller’s page, confidence should remain low.
Caffeine, Tea, and Coffee After 60
Caffeine reliably increases alertness and can reduce perceived fatigue for several hours. The FDA’s caffeine guidance emphasizes that sensitivity and product amounts vary. Caffeine does not cure the cause of brain fog, and more is not necessarily better. Older adults may clear it more slowly, so a late-afternoon cup can improve today’s alertness but impair tonight’s sleep and tomorrow’s concentration.
Coffee and tea contain many compounds, but their immediate nootropic effect is mainly caffeine. Track serving size because “one coffee” may range from a small home cup to a large café drink. Watch for tremor, anxiety, reflux, urinary urgency, palpitations, higher blood pressure, headache, and insomnia. Decaffeinated products still contain small amounts.
Interactive caffeine test: for seven days, record the time, approximate caffeine amount, alertness two hours later, bedtime, sleep quality, and next-morning clarity. Separating caffeine from protein, sweeteners, and total nutrition is easier with this practical review of clear protein and protein coffee after 60. If afternoon caffeine helps briefly but worsens the next day, move it earlier or reduce it.

Mushroom Coffee and Lion’s Mane: Promising or Proven?
Mushroom coffee usually combines coffee with powders or extracts from lion’s mane, chaga, cordyceps, reishi, or other fungi. A PubMed search of human lion’s-mane cognition studies shows why the evidence must be matched to the exact preparation and population. Species, part used, extraction method, caffeine amount, dose, contaminants, and added ingredients vary, so a standardized research extract cannot automatically validate a commercial coffee blend.
Lion’s mane has biological plausibility and small human studies, but evidence is not strong enough to conclude that it prevents cognitive decline or reliably treats brain fog after 60. Trials may use concentrated extracts at amounts unlike a beverage. Chaga may contain high oxalate levels; reishi and other extracts may affect bleeding, blood pressure, glucose, immunity, or the liver. Mushroom allergy is also possible.
If you still want to try mushroom coffee, choose a product that identifies each species, botanical part, extract amount, caffeine amount, lot number, and independent contaminant testing. Avoid proprietary blends and disease claims. Treat it as a beverage experiment, not a dementia strategy, and review it with a pharmacist when using anticoagulants, diabetes medicines, immune-modifying drugs, or multiple prescriptions.

Creatine Monohydrate for Memory and Mental Fatigue
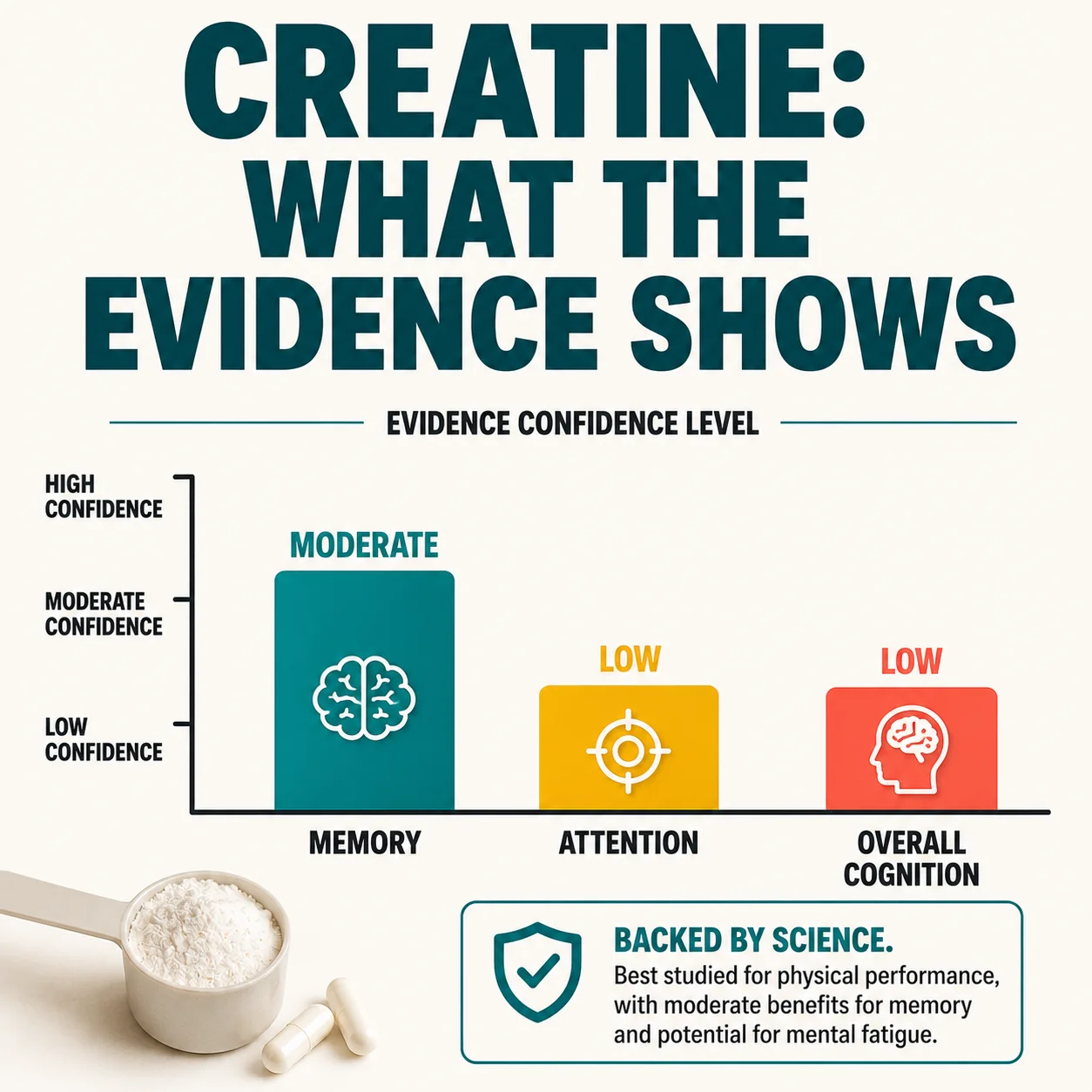
Creatine helps buffer cellular energy through the creatine–phosphocreatine system. A 2024 systematic review and meta-analysis of randomized trials reported possible benefits for memory, attention time, and processing speed, while other cognitive outcomes remained uncertain. Results are inconsistent, brain uptake is regulated, and “brain fog” is not a standardized research outcome.
Plain creatine monohydrate is the research standard. There is no FDA-approved brain-fog dose. Many adult routines use a maintenance amount without a loading phase, but adults over 60 should discuss kidney history, heart failure, fluid restrictions, medicines, and laboratory monitoring first. Creatine can raise serum creatinine and complicate interpretation of a creatinine-derived eGFR without automatically proving kidney injury; a changed result still requires clinical interpretation.
A reasonable trial measures a functional outcome for six to eight weeks: sustained reading, list recall, error rate, or afternoon task completion. Do not judge it by a stimulant-like sensation. Stop for concerning swelling, reduced urination, severe digestive symptoms, rapid unexplained weight change, or a clinician-directed laboratory concern.
Ginkgo, Bacopa, Huperzine A, and Other Brain Herbs
The NCCIH evidence summary for ginkgo reports that it has not been shown to prevent dementia reliably or consistently improve cognition in healthy people. It may increase bleeding risk and interact with anticoagulants, antiplatelet drugs, seizure medicines, and other products. “Improves circulation” is not a sufficient reason to use it.
Bacopa has small studies suggesting possible memory effects, but preparations and doses vary, gastrointestinal effects are common, and evidence specific to U.S. adults over 60 is limited. Huperzine A affects acetylcholine signaling and can cause nausea, sweating, slowed heart rate, vivid dreams, or interactions; it should not be casually stacked with dementia medicines or anticholinergic drugs.
Rhodiola, ashwagandha, phosphatidylserine, acetyl-L-carnitine, and other ingredients each have different evidence and risks. Combining them does not make the evidence additive. It makes cause and side effects harder to identify. If a product needs a dense panel of ingredients to sound convincing, that is usually a reason to slow down.
Vitamins, Omega-3s, and Deficiency-Targeted Treatment
Deficiency-targeted treatment can work when the deficiency is real. The NIH Office of Dietary Supplements’ vitamin B12 fact sheet explains that deficiency can affect blood cells and the nervous system. Treatment matters when testing and clinical context support it. Folate, iron, thyroid hormone, or vitamin D should likewise address a documented problem or clinician-defined indication, not a vague promise of mental energy.
High-dose B vitamins do not reliably sharpen cognition in people who are already replete, and vitamin B6 excess can injure nerves. Omega-3 fats are important nutrients, but supplement trials have not established fish-oil capsules as a universal memory treatment. Food patterns rich in fish, plants, beans, nuts, whole grains, and unsaturated fats support cardiovascular health without depending on one capsule.
Before assuming a nutritional shortfall is clouding your focus, review your daily habits and consider choline-rich foods for memory after 60. Whole foods such as eggs or poultry can support balanced intake, while healthier dietary fats for cognitive and cardiovascular support belong in the same food-first discussion with a clinician. Ask which deficiency is suspected, how testing would change treatment, and avoid panels sold by companies whose answer is always another supplement.
Cognitive Training: What Transfers to Daily Life?
Cognitive training can improve practiced skills. The National Institute on Aging’s review of cognitive training describes encouraging results alongside uncertainty about broad protection. Speed practice may improve speed tasks, and memory strategies may improve recall methods, but transfer to everyday cognition is smaller and less certain. A high game score does not prove reduced dementia risk.
Training becomes more useful when it resembles the desired function. If the goal is remembering medicines, practice a pill-organizer routine with alarms and teach-back. If the goal is names, practice spaced retrieval using real people. If the goal is navigation, safely rehearse routes with a partner rather than tapping abstract shapes.
Interactive training plan: choose one daily-life target, practice 20–30 minutes three times weekly, and test the real task once weekly. Increase difficulty gradually. Stop if the program causes headaches, frustration, sleep loss, or unsafe confidence. Learning music, a language, dance steps, volunteering procedures, or technology may offer cognitive challenge plus meaning and social contact.
Exercise, Sleep, Hearing, and Cardiovascular Brain Health
Exercise is a multi-system brain intervention. The U.S. government’s Physical Activity Guidelines for Americans supports aerobic, muscle-strengthening, and balance activity for older adults according to ability. KeepFitQuote’s guides to muscle mass and metabolic rate after 60 and fruit choices that support mobility and muscle health help translate that foundation into daily routines. Start appropriately and seek clearance when symptoms make exercise unsafe.
Sleep supports attention and memory consolidation. Loud snoring, gasping, witnessed pauses, morning headaches, resistant hypertension, and daytime sleepiness warrant screening for sleep apnea. Hearing and vision correction reduce cognitive load and improve access to information. Social isolation, depression, grief, and chronic pain deserve direct treatment rather than stimulation.
Readers using wearables can use KeepFitQuote’s decision guide to low HRV and poor deep sleep after 60 without treating device estimates as diagnoses. Its review of left-side sleeping after 60 also separates possible comfort or reflux benefits from conditions that need clinical care. Cardiovascular risk factors remain brain-health factors; no supplement can compensate for ignoring them.
Medication and Supplement Safety After 60
Older adults are more likely to use multiple medicines and have changes in kidney or liver function. The FDA warns that mixing medicines and dietary supplements can be dangerous, making dose, duplication, and interaction review essential. Bring the exact bottles or clear label photographs to a pharmacist, including gummies, powders, teas, energy drinks, sleep aids, CBD products, and “natural” remedies.
High-risk combinations include multiple stimulants; ginkgo or concentrated herbs with anticoagulants; sedating blends with opioids or sleep medicines; blood-pressure-lowering herbs with antihypertensives; and glucose-lowering products with diabetes medicines. Surgery and procedures may require advance discontinuation of certain supplements, but the surgeon should set the plan.
The FDA’s information for supplement consumers explains that supplements are not approved for effectiveness before marketing. Report serious reactions through FDA MedWatch and seek urgent care for severe symptoms.

Older-Adult Interaction and Contraindication Check
| Situation | Why It Matters | Safer Next Step |
|---|---|---|
| Anticoagulant or antiplatelet therapy | Ginkgo and some botanicals may increase bleeding risk | Pharmacist review before any herb or blend |
| Blood-pressure or heart-rhythm treatment | Stimulants may affect pressure, pulse, sleep, or symptoms | Review caffeine and every stimulant ingredient |
| Diabetes medicines | Some herbs may alter glucose and complicate dosing | Monitor only under the diabetes-care plan |
| Kidney or liver disease | Clearance, toxicity, and laboratory interpretation may change | Avoid self-starting; obtain condition-specific advice |
| Psychiatric, seizure, or sleep medicines | Activation, sedation, or neurotransmitter effects may interact | Use a complete medicine-and-supplement review |
| Surgery or procedure planned | Bleeding, sedation, pressure, and glucose effects can matter | Give the surgical team the exact product list early |
Do not stop prescription medicines or preoperative supplements without instructions from the prescribing or surgical team.
How to Read a Nootropic Label in the USA
Use the five-line label test. The FDA’s questions and answers about dietary supplements clarifies U.S. labeling and regulatory responsibilities. Ask whether every active ingredient and amount is disclosed, caffeine is stated per serving, credible independent verification exists, and the claims stop short of promising to cure disease.
Avoid “proprietary blends,” aggressive before-and-after claims, fake clinician imagery, countdown timers, and language promising to reverse Alzheimer’s disease. Search the exact product and company with the words warning, recall, FDA, lawsuit, and adverse event. Independent certification does not prove effectiveness, but it can reduce uncertainty about identity and contamination.
Choose one-ingredient products when testing one hypothesis. Keep the lot number and receipt. Do not buy a year’s supply before learning whether the product is tolerable or useful.
Interactive Nootropic Decision Scorecard
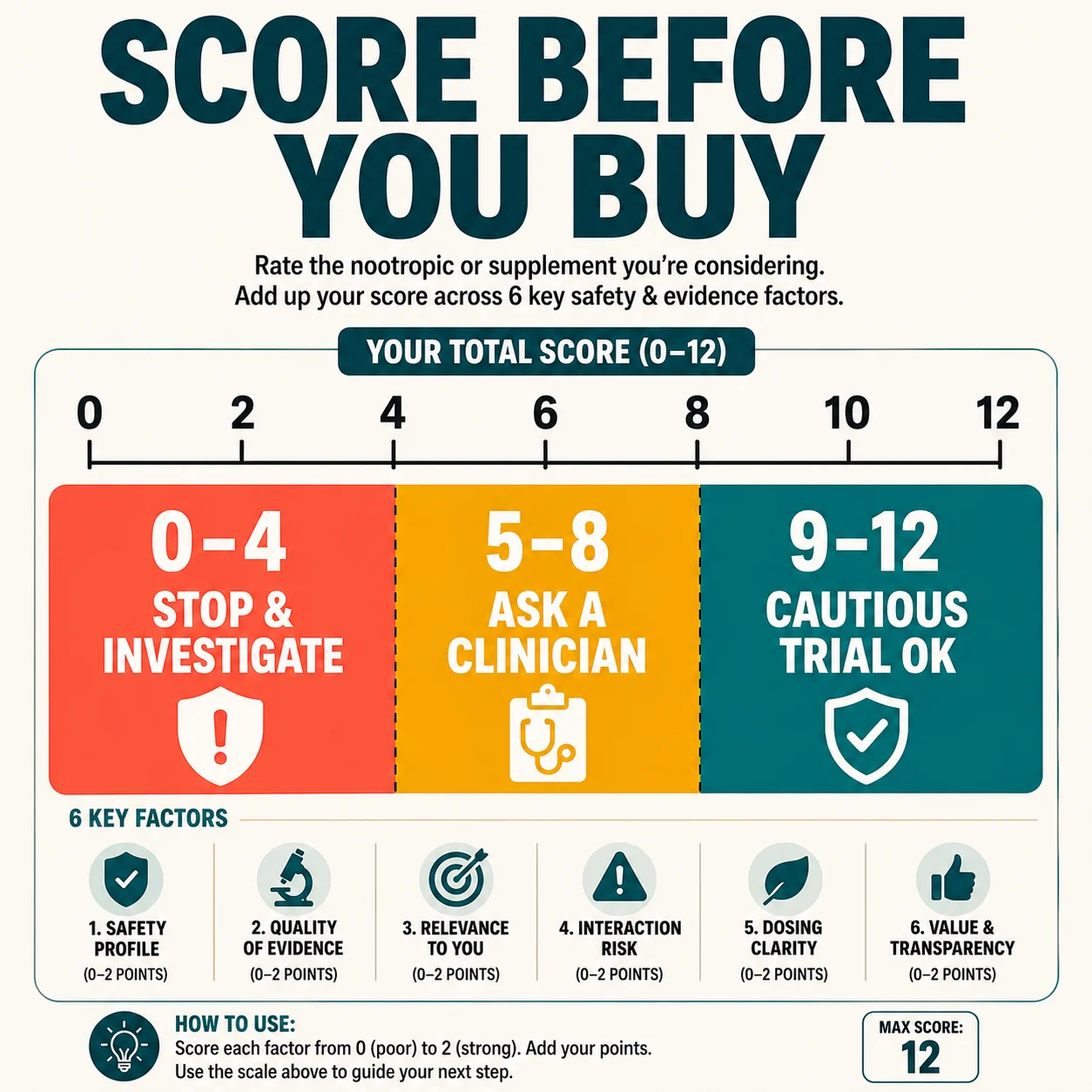
Score each item 0, 1, or 2. The NCCIH consumer guide to using dietary supplements wisely supports checking evidence, safety, and professional guidance before buying. A total of 0–4 means stop and investigate first; 5–8 means discuss with a clinician or pharmacist; 9–12 means a cautious one-variable trial may be reasonable if no red flags exist.
Clear target: 0 vague promise; 1 symptom defined; 2 one functional outcome defined.
Evidence: 0 testimonials; 1 small or indirect studies; 2 repeated relevant human evidence.
Safety: 0 unknown interactions; 1 partial review; 2 complete medicine and condition review.
Product quality: 0 hidden blend; 1 transparent label; 2 transparent plus credible independent testing.
Measurement: 0 feelings only; 1 symptom score; 2 baseline plus repeated real-world task.
Stopping rule: 0 none; 1 vague; 2 specific date, side-effect rule, and no-benefit rule.
Reader decision: write the score before buying. Marketing excitement should not change it. If the score rises only because the seller made a claim, the evidence has not actually improved.
A Six-Week One-Variable Trial
Week 0: establish baseline. The NIH Clinical Center explains why controlled comparisons matter, and a personal experiment should likewise reduce avoidable confounding. Choose one outcome, repeat the same task three times, and record sleep, caffeine, alcohol, illness, stress, and medicines. Weeks 1–2: begin one clinician-approved product without simultaneously changing diet, exercise, and sleep supplements.
Weeks 3–5: keep timing and routine steady. Record weekly function and side effects, not hourly impressions. Ask a family member whether a practical change is visible. Week 6: compare averages with baseline. A true benefit should be repeatable, useful, and large enough to matter.
Stop if there is no meaningful functional improvement, if the burden outweighs the benefit, or if adverse effects appear. Do not respond to a weak result by stacking more ingredients. A negative trial is useful information.

When to Stop and Seek Medical Help
The CDC instructs people with possible stroke symptoms to call 911. Call immediately for sudden neurological symptoms, severe chest symptoms, collapse, seizure, or inability to stay awake. Seek prompt care for rapidly developing confusion, hallucinations, fever, dehydration, a fall or head injury, repeated low blood sugar, major personality change, or inability to manage medicines and basic needs safely.
Stop the product and obtain advice for new palpitations, fainting, marked blood-pressure change, serious rash, breathing difficulty, jaundice, dark urine, reduced urination, severe vomiting or diarrhea, unusual bleeding, agitation, or significant insomnia. Bring the product and medication list.
Schedule an assessment for symptoms that persist, worsen, or interfere with function. Supplements should never delay evaluation for depression, sleep apnea, thyroid disease, anemia, B12 deficiency, medication effects, mild cognitive impairment, or dementia.
FAQs: Nootropics and Brain Supplements After 60
The answers below apply the FDA’s consumer framework for dietary supplements and current U.S. healthy-aging guidance to common nootropic questions. Each answer is educational and should be individualized with a clinician or pharmacist when medicines or chronic conditions are involved.
No single nootropic reliably improves every type of cognition after 60. The National Institute on Aging’s cognitive-health guidance supports addressing medical conditions and modifiable foundations rather than relying on commercial blends.
There is no universally safest nootropic for seniors. The FDA recommends discussing supplements with healthcare professionals, because a low-risk choice must match the person’s medicines, kidneys, liver, heart, sleep, and diagnoses.
Mushroom coffee has not been proven to improve memory in older adults. The limited human lion’s-mane cognition literature indexed by PubMed cannot validate every beverage, dose, extract, or blend.
Lion’s mane may be tolerated by some adults, but older-adult safety data are limited. The NCCIH supplement-safety framework supports reviewing allergy, bleeding, glucose, immune, and medication concerns before use.
Caffeine can temporarily improve alertness and reaction time. The FDA notes that caffeine sensitivity and content vary, while anxiety, tremor, reflux, palpitations, blood pressure, urinary symptoms, or impaired sleep can erase the benefit.
Creatine monohydrate may modestly improve selected memory or attention outcomes in some people. A meta-analysis of randomized cognitive trials found encouraging signals but does not establish creatine as a treatment for brain fog, cognitive impairment, or dementia.
Ginkgo has not been shown to prevent dementia reliably. The NCCIH ginkgo review also describes safety and interaction concerns, including bleeding risk for people using anticoagulants or antiplatelet drugs.
Brain-training games can improve practiced skills, but broad transfer is uncertain. The National Institute on Aging’s discussion of cognitive training supports cautious expectations rather than promises of dementia prevention.
A vitamin helps cognition mainly when it corrects a relevant deficiency or medical problem. The NIH vitamin B12 fact sheet explains deficiency risks, while high-dose vitamins do not reliably sharpen memory in already well-nourished adults.
Fish oil is marketed as a nootropic, but capsules are not a universal memory treatment. The NIH omega-3 fact sheet provides evidence and safety context for discussing bleeding risk, diet, cardiovascular indications, and medicine interactions.
Yes, several herbs and blends may increase bleeding risk or alter drug effects. The FDA’s medicine-and-supplement warning supports pharmacist review before combining any supplement with a blood thinner.
Stimulant ingredients can raise blood pressure or heart rate in some people. The FDA’s caffeine guidance helps frame caffeine exposure, while yohimbe-like ingredients and undisclosed drug analogs warrant additional caution.
Use a defined trial long enough to match the intervention, commonly several weeks rather than one dose. The NCCIH guide to supplements emphasizes evidence and safety; set duration with a clinician and stop for adverse effects or no meaningful benefit.
Do not begin with a nootropic stack. The FDA warns that supplement–medicine combinations can cause harmful effects, and multiple new ingredients make benefits or adverse effects impossible to attribute.
Brain fog needs evaluation when it is sudden, progressive, function-limiting, associated with neurological signs, or noticed by family. The CDC’s stroke guidance identifies emergency warning signs that require 911 rather than a supplement trial.
The Bottom Line on Nootropics After 60
What really works after 60 is rarely a secret ingredient. The National Institute on Aging identifies modifiable cognitive-health factors that include medical care, physical activity, sleep, sensory health, and engagement. The most dependable strategy is to identify the cause of symptoms, strengthen cardiovascular health, correct documented deficiencies, and use training that resembles the desired daily task.
Caffeine can help short-term alertness; creatine may help selected people and outcomes; cognitive training can improve practiced abilities. Mushroom coffee, lion’s mane, ginkgo, bacopa, and multi-ingredient brain blends remain uncertain or carry meaningful interaction concerns. A product should earn its place through transparent ingredients, relevant human evidence, medical compatibility, and a measurable benefit—not clever branding.
Use the ring-fence rule: one target, one intervention, one baseline, one trial period, and one stopping rule. If symptoms are sudden, worsening, or affecting safety, the right next step is medical care, not a stronger stack.
Keep the goal human. The purpose is not to collect the most sophisticated supplement routine or achieve a perfect game score. It is to read, converse, plan, remember commitments, manage health tasks, and participate in daily life with greater safety and confidence. When an intervention does not improve those priorities, its biochemical story and marketing vocabulary do not make it valuable.
Authoritative U.S. Resources
- National Institute on Aging: Cognitive Health and Older Adults
- FDA: Information for Consumers Using Dietary Supplements
- FDA: How to Spot Health Fraud
- CDC: Signs and Symptoms of Stroke
- NCCIH: Herbs at a Glance
Medical disclaimer: This article provides general education for U.S. adults and does not diagnose, prescribe, or replace individualized care. Dietary supplements are not FDA-approved to treat brain fog, cognitive decline, or dementia. Call 911 for emergency symptoms.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.







