Low HRV and Poor Deep Sleep After 60: When to Worry
A practical guide to understanding smartwatch and smart-ring readings, checking likely causes, and knowing when to seek medical help.
One low HRV or poor deep-sleep reading after 60 is usually not an emergency. Compare a 7- to 14-day trend with your own baseline. Contact a clinician if the change persists with fatigue, snoring, gasping, palpitations, dizziness, or breathlessness. Call 911 for chest pain, fainting, severe breathing trouble, or stroke symptoms. Wearables show patterns; they do not diagnose disease.
Wearable Device Symptom Check for Older Adults
To evaluate your metrics alongside the health and recovery frameworks outlined by the National Institute on Aging guidance on older-adult sleep patterns, choose the statement below that best maps to your current real-world situation.
One odd night, no symptoms: Check the fit of the device, think about yesterday’s stressors, and watch the next few nights.
Several low nights, but you feel normal: Standardize how you measure, review common triggers, and look at a 7- to 14-day trend.
Persistent change plus fatigue, snoring, palpitations, or breathlessness: Arrange a medical appointment and bring the trend report and medication list.
Chest pain, fainting, severe shortness of breath, stroke symptoms, or marked confusion: Call 911 or obtain emergency care now. Do not wait for the wearable to confirm anything.
This guide explains why those four paths are different.
What HRV Actually Measures
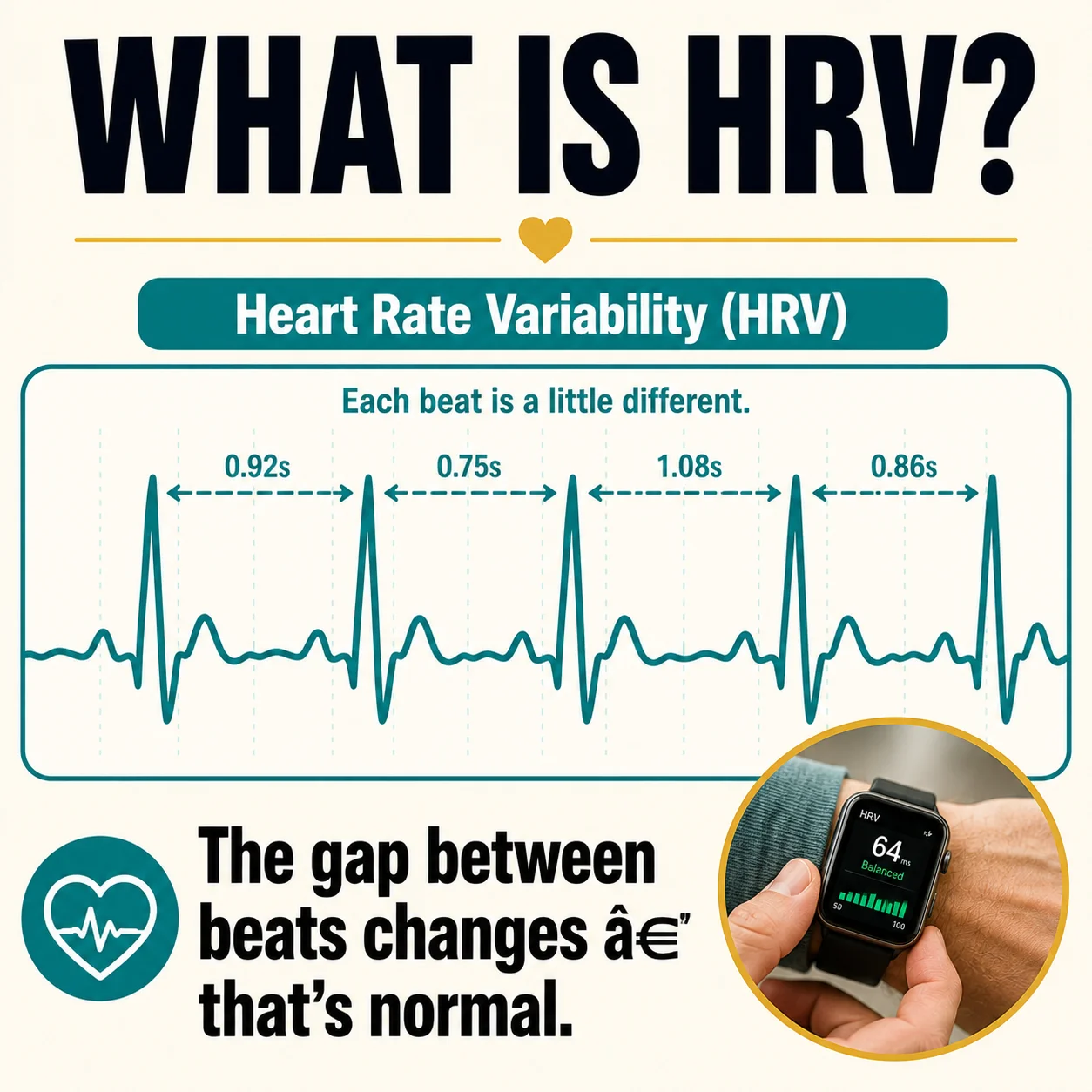
Your heart does not beat like a perfectly timed metronome. Even at a steady pulse of 60 beats per minute, the gap between one beat and the next changes slightly. Heart rate variability describes this beat-to-beat variation, usually measured in milliseconds; peer-reviewed smartwatch HRV research documents differences in sensors, algorithms, and measurement windows.
HRV reflects the interaction of the autonomic nervous system’s two main branches. The sympathetic branch helps the body respond to effort, threat, pain, and stress. The parasympathetic branch supports rest, digestion, and recovery. In general, higher HRV relative to your personal baseline can accompany good recovery and flexible nervous-system regulation. Lower HRV can occur when the body is under strain.
That does not make “high” automatically healthy or “low” automatically dangerous. HRV varies with age, genetics, fitness, breathing, posture, sleep stage, time of day, illness, medications, and the mathematical method used. One device may report RMSSD, another SDNN, and another a proprietary “readiness” score. Values from different brands may not be directly comparable.
For adults over 60, comparing a reading with an online table can be misleading. The better comparison is with measurements collected by the same device, under similar conditions, over time. Your normal may be lower than a younger athlete’s and still be appropriate for you.
Why Wearable HRV Numbers Differ: RMSSD, SDNN, PPG and ECG
Wearables do not all calculate HRV the same way. RMSSD emphasizes short-term beat-to-beat variation and is commonly used for overnight recovery. SDNN summarizes overall variation across the measurement window. A value from one metric, device, or sampling period should not be compared directly with another.
Most watches and rings use photoplethysmography (PPG), which estimates pulse timing from light reflected through the skin. Clinical electrocardiography (ECG) measures the heart’s electrical signal and remains the reference method for rhythm assessment. Motion, loose fit, cold skin, poor circulation, irregular beats, and algorithm changes can alter PPG-derived results.
For useful trend tracking, use the same device, wear position, measurement window, and routine. Record the device model and metric when sharing results with a clinician. A wearable trend can support a conversation, but an ECG, rhythm monitor, or sleep study may be needed when symptoms or repeated alerts are present.
What “Poor Deep Sleep” Means on a Wearable
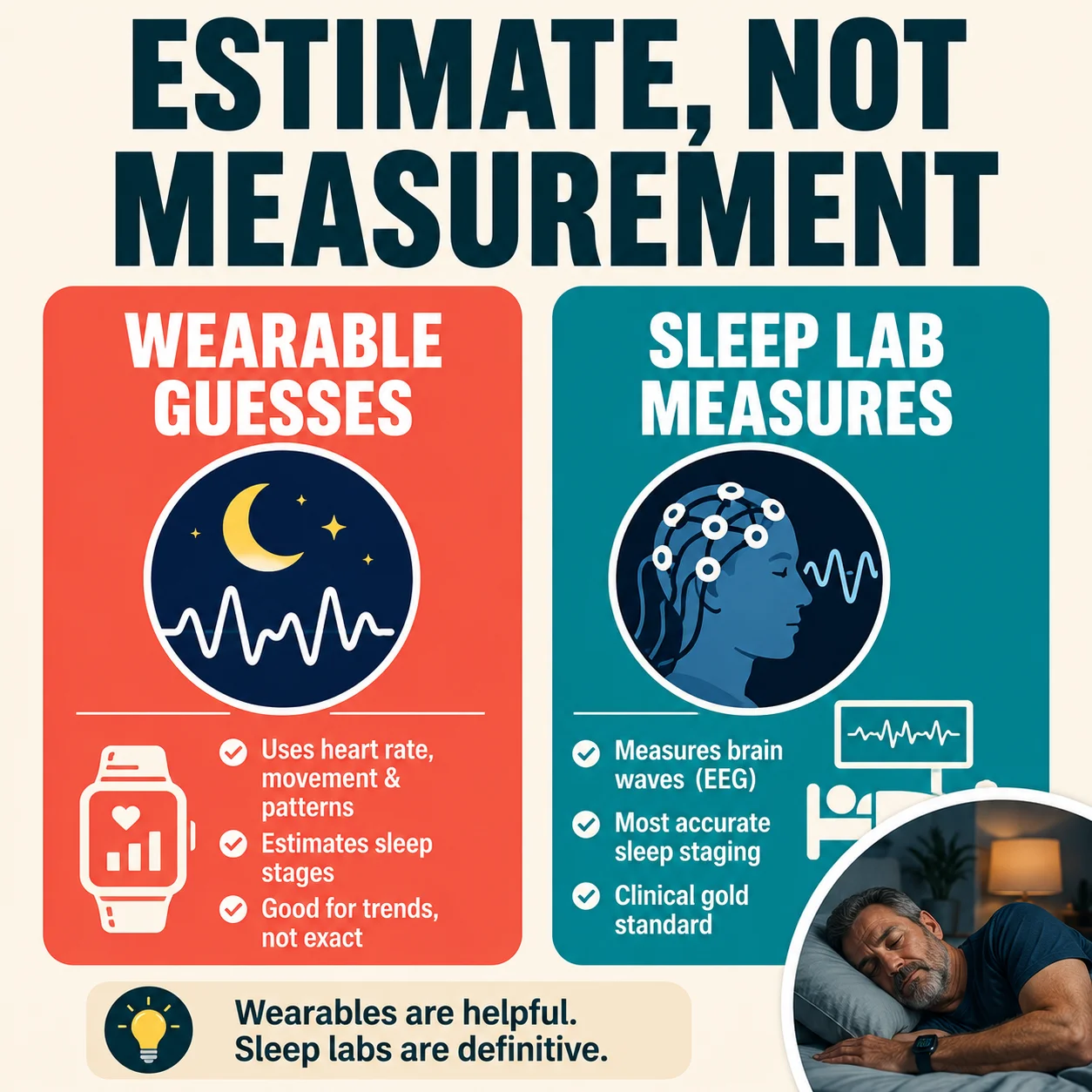
Deep sleep describes stage N3 non-rapid-eye-movement sleep, also called slow-wave sleep. During laboratory polysomnography, clinicians identify sleep stages using brain waves, eye movements, muscle activity, breathing, oxygen levels, and heart rhythm. Validation studies of consumer sleep wearables demonstrate that wrist-worn devices are highly effective for tracking broad overnight trends, even though their specific sleep-stage estimates remain strictly approximate. Older adults can implement specific adjustments for sleeping more continuously without treating tracker estimates as a medical diagnosis.
Most consumer watches and rings do not measure brain waves. They infer sleep stages from movement, pulse patterns, HRV, breathing signals, temperature, and algorithms. That distinction matters. A device may be reasonably useful for noticing bedtime, wake time, or broad trends while still confusing deep, light, REM, and awake periods.
In a validation study comparing six wearables with laboratory measures, performance varied substantially by device. Some devices identified sleep better than wakefulness, and sleep-stage agreement was generally less dependable than basic sleep/wake detection. A 2024 study likewise reported high sensitivity for detecting sleep but much lower sensitivity for distinguishing particular sleep stages. Recent research also suggests consumer devices may be less accurate for some measurements in older adults than in younger adults. These findings do not make wearables useless; they define the correct use: trend detector, not sleep laboratory.
Deep sleep naturally changes with aging. Older adults often have lighter, more fragmented sleep and less N3 sleep than younger adults. Therefore, a small deep-sleep percentage after 60 is not automatically evidence of disease. How you function during the day and whether the pattern changed from your baseline are often more informative than a single percentage.
Why Low HRV and Poor Deep Sleep After 60 May Appear Together
HRV and sleep are connected because both respond to the autonomic nervous system, breathing, recovery, and health stressors. When sleep is repeatedly interrupted, the body may spend more time in an alert state. Conversely, illness, pain, alcohol, emotional strain, or breathing problems may lower HRV while also fragmenting sleep; sleep-tracker validation research supports using multi-night trends instead of exact stage minutes.
Common short-term explanations include: emotional stress, grief, anxiety, or an unusually demanding day; alcohol, especially within several hours of bedtime; a large or late evening meal; dehydration, fever, infection, or recovery from illness; vigorous exercise without adequate recovery; travel, jet lag, an unfamiliar room, or a changed schedule; pain, nighttime urination, reflux, coughing, or hot flashes; caffeine late in the day or nicotine use; a new medication, dose change, or interaction; and poor sensor contact, low battery, movement, cold skin, or an algorithm update.
Longer-lasting patterns may be associated with sleep apnea, chronic insomnia, persistent pain, depression or anxiety, thyroid disease, diabetes, cardiovascular disease, an abnormal heart rhythm, lung disease, medication effects, or deconditioning. The wearable pattern cannot determine which cause is present. Symptoms, medical history, examination, and appropriate testing do that.
Low HRV Cause, Clue and First Action
Use this quick pattern check to choose a sensible first step. More than one factor may apply, and none of these patterns is a diagnosis.
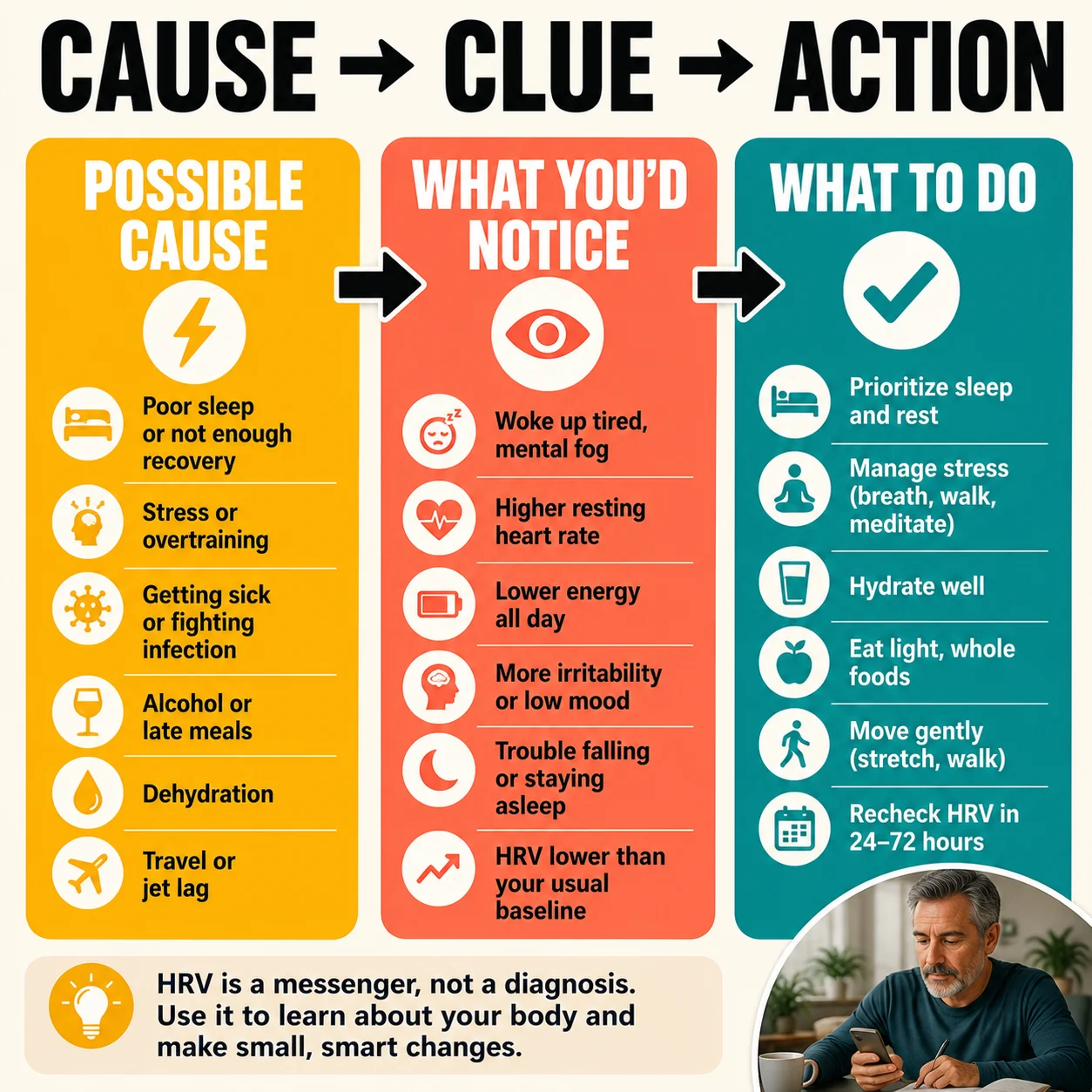
| Possible Cause | Clues | First Action |
|---|---|---|
| Measurement noise | Missing data, implausible spikes, loose fit, or a changed device | Refit the sensor and repeat under normal conditions |
| Stress, alcohol, or late eating | A temporary drop after an unusual evening | Remove the trigger and compare several similar nights |
| Illness or dehydration | Fever, cough, stomach illness, dark urine, rising resting heart rate, or unusual fatigue | Recover, hydrate as medically appropriate, and contact a clinician if symptoms persist |
| Training overload | Soreness, reduced performance, poor sleep, and low HRV after harder activity | Reduce intensity briefly and reassess recovery |
| Sleep-disordered breathing | Loud snoring, witnessed pauses, gasping, morning headache, or daytime sleepiness | Request sleep-apnea screening |
| Possible rhythm or cardiovascular problem | Repeated irregular-rhythm alerts, palpitations, dizziness, fainting, chest pressure, or breathlessness | Seek timely medical evaluation; call 911 for emergency symptoms |
The Three-Question Method: Reading, Trend, Symptoms
When a low number appears, walk through three questions in order; National Institute on Aging fatigue guidance advises investigating persistent tiredness rather than attributing it to age alone.
1. Could the Reading Be Unreliable?
Check whether the device was snug but comfortable and positioned as the manufacturer recommends. Look for missing data, unusual gaps, a very low battery, a recently changed wrist or finger, swelling, cold hands, or a software update. Movement and poor skin contact can disturb optical pulse measurements. Differences in skin properties, circulation, tattoos, device location, and sensor design may also affect performance; peer-reviewed wearable studies find stronger performance for sleep detection than for precise stage classification.
Do not compare an overnight ring value with a morning reading from a chest strap or another brand as though they are identical. Use the same device and measurement window. If the device provides raw heart-rate traces, look for gaps or obvious spikes. Repeat the measurement under normal conditions before building a medical conclusion around it.
2. Is This a Real Trend for You?
One point is noise; a repeated departure from baseline is a signal worth interpreting. Examine at least seven nights when practical, and preferably two to four weeks. Compare the recent median or weekly average with your usual range. Note whether resting heart rate rose at the same time, whether sleep duration shortened, and whether the change followed illness, travel, alcohol, increased training, or a medication adjustment; wearable HRV research shows that personal trends are more interpretable than cross-device comparisons.
Avoid inventing a universal cutoff. A value of 20 milliseconds may be ordinary for one person and a marked decline for another. Equally, an apparently “good” number cannot rule out disease. Your device’s consistent trend is more useful than a leaderboard.
3. Are Symptoms or Warning Signs Present?
The medical importance rises when the wearable change agrees with the body’s message. New daytime sleepiness, exhaustion, reduced stamina, repeated awakenings, loud snoring, witnessed pauses in breathing, choking or gasping, morning headaches, palpitations, dizziness, swelling, shortness of breath, or chest pressure deserve attention; American Heart Association guidance identifies chest pressure, severe breathlessness, fainting, and neurologic change as urgent warning signs.
Symptoms override the score. If you feel seriously unwell, do not delay care because an app says your recovery is “fair.” If you feel well and one night is abnormal, do not panic because a dashboard turns red.
When It Is Probably Just a Wearable Reading
Consumer sleep-wearable studies show that sensor conditions can distort stage estimates, so observation is generally reasonable when all of the following are true: the low HRV or low deep-sleep estimate occurred for only one or two nights; you have no chest pain, fainting, unusual breathlessness, new confusion, or neurologic symptoms; you feel close to your normal self during the day; there is a plausible temporary trigger, such as alcohol, travel, stress, illness, pain, or hard exercise; resting heart rate and other measurements are not showing a major unexplained change; the device had questionable fit, incomplete data, or another possible measurement problem; and the reading begins returning toward your normal range after recovery.
This is not a guarantee that nothing is wrong. It is a reasonable way to avoid treating a consumer estimate as a diagnosis. Continue observing your symptoms and trends.
When to Schedule a Routine Medical Appointment
American Heart Association arrhythmia guidance recommends symptom review and ECG-based monitoring for suspected rhythm problems. Contact your primary care clinician when low nighttime HRV or poor deep sleep persists, differs clearly from baseline, or changes how you function, especially if you notice: a downward HRV trend lasting roughly one to two weeks without an obvious explanation; poor sleep and daytime impairment occurring at least several times a week; new exercise intolerance or recovery that is consistently worse; loud snoring, witnessed breathing pauses, gasping, morning headaches, or dry mouth; frequent nighttime urination combined with snoring or daytime sleepiness; recurrent palpitations or irregular-rhythm notifications without severe symptoms; a recent medication or dose change followed by sleep or heart-rate changes; persistent pain, low mood, anxiety, or restless legs disrupting sleep; or increasing resting heart rate, blood pressure, or glucose alongside declining sleep.
The precise number of days is not a medical cutoff. It is a practical threshold for turning scattered readings into a usable trend. People with known heart disease, atrial fibrillation, heart failure, COPD, diabetes, prior stroke, or sleep apnea should follow their clinician’s personalized advice and may need earlier contact.
When to Seek Urgent or Emergency Help
In alignment with the American Heart Association emergency guidance regarding immediate cardiac care, our guide to early heart-attack symptoms in seniors provides an essential breakdown of physical warning patterns older adults must never dismiss. Call 911 in the United States if a low HRV or abnormal sleep report occurs with any of the following: chest pain, pressure, squeezing, or discomfort—particularly with sweating, nausea, or pain in the arm, back, neck, or jaw; severe or sudden shortness of breath; fainting, near-fainting, or inability to stand safely; a sustained rapid or markedly irregular heartbeat with weakness, chest discomfort, or lightheadedness; sudden facial droop, arm weakness, speech difficulty, loss of balance, or severe new headache; or new marked confusion, inability to awaken normally, or bluish lips.
Do not drive yourself if symptoms are severe. Do not spend time recalibrating the wearable, searching for a better HRV score, or waiting for another night of data. Emergency decisions are based on symptoms and clinical risk, not a consumer sleep score.
Sleep Apnea: The Important Connection After 60
Obstructive sleep apnea causes repeated narrowing or closure of the upper airway during sleep. Breathing may stop or weaken, oxygen may fall, and the brain briefly activates to reopen the airway. These repeated stress responses can fragment sleep and alter heart-rate patterns even when the person does not remember waking; NHLBI sleep-apnea guidance identifies loud snoring, gasping, and observed breathing pauses as screening triggers.
Risk increases with age, but body size alone does not determine who develops apnea. Warning signs include loud habitual snoring, observed pauses, choking or gasping, unrefreshing sleep, morning headache, dry mouth, nighttime urination, daytime sleepiness, difficulty concentrating, resistant high blood pressure, and atrial fibrillation.
A wearable may flag oxygen changes, breathing disturbances, low deep sleep, or unusual pulse patterns. These clues can justify a conversation, but they do not establish or exclude sleep apnea. Diagnosis usually requires a home sleep apnea test or an overnight laboratory study ordered and interpreted by a qualified clinician. A “normal” wearable night should not overrule convincing symptoms.
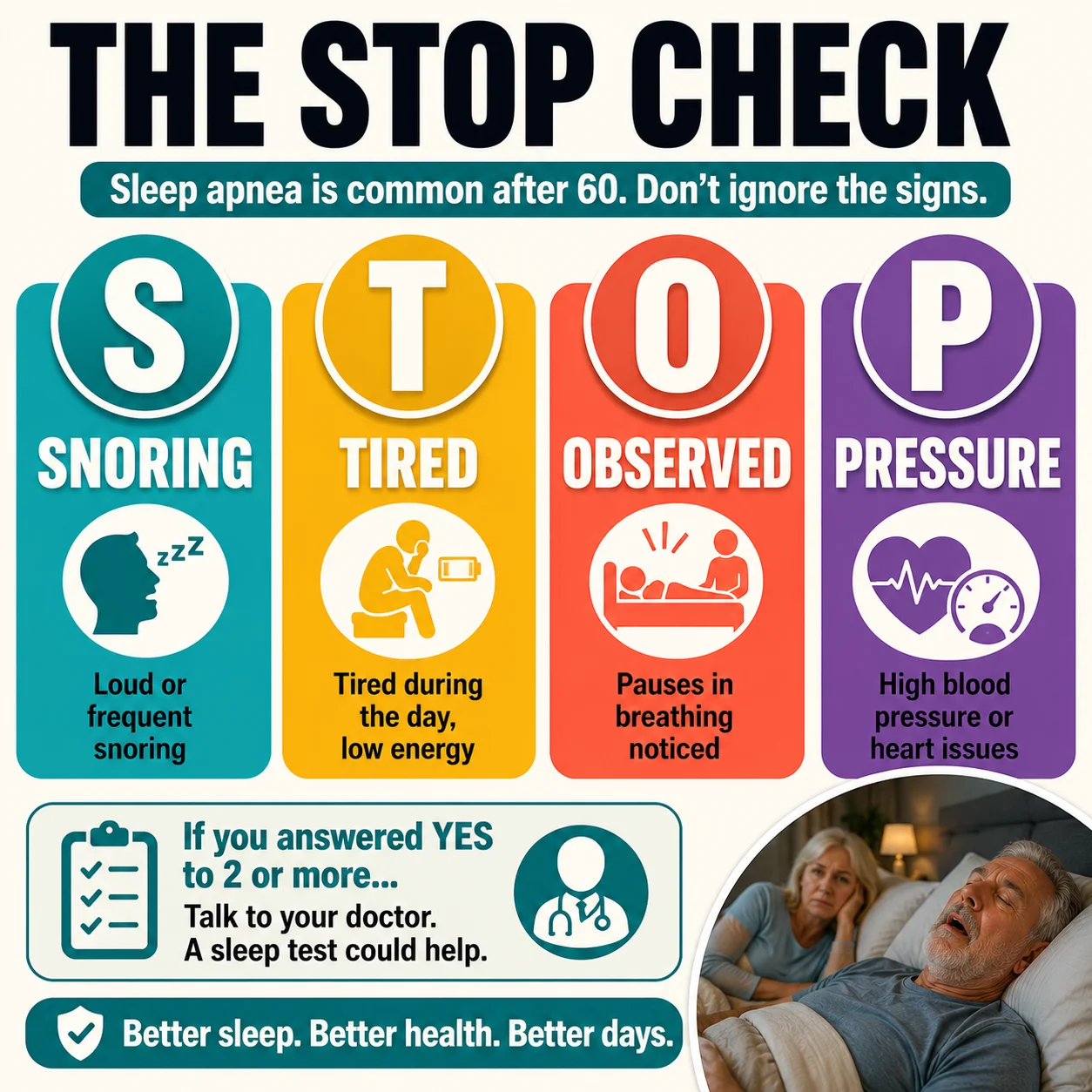
Interactive STOP Check
NHLBI sleep-apnea guidance identifies snoring, gasping, breathing pauses, and daytime sleepiness as screening triggers, so ask yourself four simple questions:
S — Snoring: Is it loud enough to be heard through a door or disturb another person?
T — Tired: Are you frequently sleepy, fatigued, or unrefreshed during the day?
O — Observed: Has anyone seen you stop breathing, choke, or gasp during sleep?
P — Pressure: Do you have high blood pressure or treatment that is difficult to control?
One “yes” does not diagnose apnea. Multiple “yes” answers—especially with age over 60, atrial fibrillation, obesity, or a larger neck—strengthen the case for professional screening.
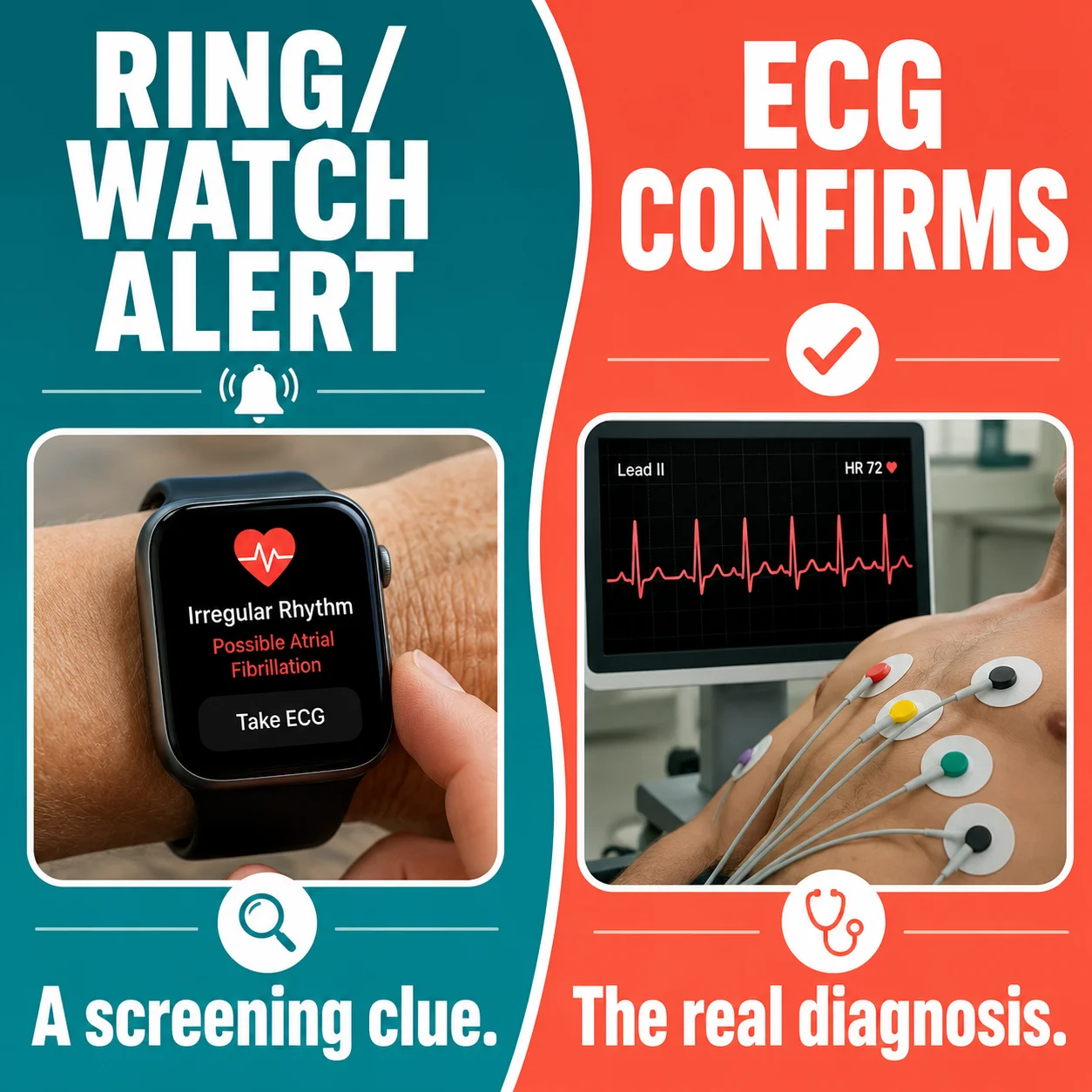
Atrial Fibrillation and Other Rhythm Concerns
Atrial fibrillation is an irregular heart rhythm that becomes more common with age and increases stroke risk. Some wearables can identify an irregular pulse pattern or record a single-lead electrocardiogram. HRV alone, however, is not an atrial fibrillation test. In fact, rhythm irregularity may produce unusual variability that an app interprets differently depending on its algorithm; American Heart Association atrial-fibrillation guidance links palpitations, dizziness, weakness, and breathlessness with timely rhythm evaluation.
Repeated irregular-rhythm notifications should be discussed with a clinician, even if you feel well. Confirmation generally requires a medical-quality ECG or longer rhythm monitor. Palpitations with fainting, chest pain, severe breathlessness, weakness, or neurologic symptoms require urgent evaluation.
If your device has an ECG feature, save a readable tracing during symptoms if you can do so safely. Do not repeatedly provoke symptoms or delay care to capture the perfect recording. Record the time, activity, duration, pulse, and associated symptoms.
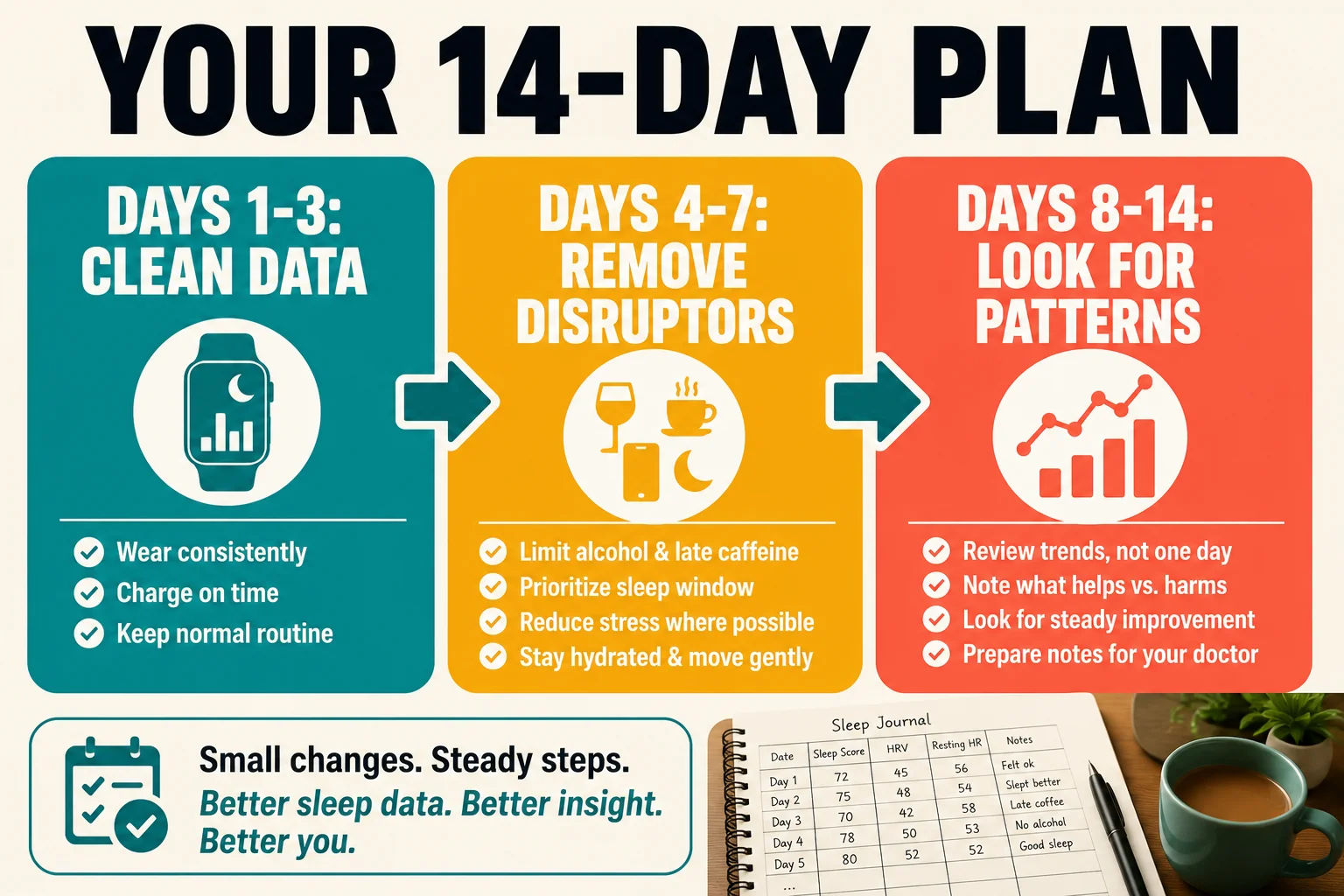
A Practical 14-Day Reset and Observation Plan
If you have no emergency symptoms and the situation is suitable for self-observation, use this two-week plan. Its purpose is not to “hack” a number; it is to improve measurement quality, remove common stressors, and produce information a clinician can use; National Institute on Aging sleep recommendations emphasize regular schedules, daytime activity, and fewer evening disruptors. You can pair this plan with these safe nighttime habits for adults over 70 and adapt the suggestions to your health and mobility.
Days 1–3: Establish Clean Data
Wear the device consistently and according to its instructions. Keep bedtime and wake time within a similar window. Do not introduce several supplements or extreme lifestyle changes. Record bedtime, wake time, alcohol, caffeine, exercise, illness, pain, medications, naps, and how refreshed you feel from 0 to 10; the National Institute on Aging recommends judging older-adult sleep by function, consistency, and symptoms.
Check the device once in the morning, then move on. Repeated checking can create anxiety and worsen sleep—a pattern sometimes called orthosomnia, in which the pursuit of perfect sleep data becomes part of the sleep problem.
Days 4–7: Remove High-Impact Disruptors
Avoid alcohol near bedtime. Stop caffeine early enough that it does not interfere with your sleep; for many people, that means avoiding it after lunch, though sensitivity varies. Finish heavy meals several hours before bed. Maintain hydration during the day while limiting excessive fluid close to bedtime if nighttime urination is a problem; the National Institute on Aging advises limiting late caffeine, alcohol, and heavy meals to protect sleep continuity.
Get morning daylight, remain physically active within your medical limits, and allow recovery after demanding exercise. Keep the bedroom dark, quiet, and comfortably cool. Create a 30- to 60-minute wind-down period with lower light and less stimulating content.
Days 8–14: Look for Patterns, Not Perfection
Review weekly medians or averages rather than the best and worst nights. National Institute on Aging sleep guidance recommends evaluating patterns across multiple nights. Use these questions: Did HRV move back toward my baseline? Did resting heart rate normalize? Did perceived sleep improve even if “deep sleep” did not? Were low nights linked with alcohol, pain, stress, illness, late food, or hard exercise? Am I sleepy while driving, forgetting routine tasks, or limiting activity because of fatigue? Did anyone observe snoring, pauses, gasping, or unusual movements?
If the trend improves and you feel well, continue the helpful habits. If it remains substantially abnormal or symptoms persist, schedule a medical review. Bring the log rather than trying to remember two weeks of details.
Preparing Smartwatch Health Logs for Your Physician
American Heart Association arrhythmia guidance recommends bringing symptoms and rhythm records to a clinical evaluation. A concise record is more useful than hundreds of screenshots, so prepare: your usual HRV range and the date the change began; a 7-, 14-, or 30-day trend from the same device; resting heart-rate trend and any ECG or irregular-rhythm notifications; typical sleep and wake times, awakenings, naps, and daytime sleepiness; snoring, gasping, morning headaches, nighttime urination, or witnessed pauses; recent infection, stress, travel, pain, exercise changes, alcohol, or dehydration; a complete list of prescriptions, over-the-counter drugs, and supplements; known diagnoses such as hypertension, diabetes, thyroid disease, COPD, atrial fibrillation, heart failure, or sleep apnea; and the question you want answered: “Could this reflect a rhythm problem, medication effect, sleep apnea, or another treatable cause?”
Your clinician may review blood pressure, pulse, heart and lung findings, medication timing, and sleep-apnea risk. Depending on the situation, testing may include an ECG, ambulatory rhythm monitor, blood count, thyroid studies, metabolic testing, or a sleep study. Not everyone needs every test.
Which Clinician Should You Contact First?
Start with the professional best matched to the pattern; your primary care clinician can coordinate referrals when the cause is unclear.
Primary care: persistent low readings, fatigue, medication changes, infection, thyroid concerns, diabetes, or several possible causes.
Sleep specialist: loud snoring, witnessed breathing pauses, gasping, severe daytime sleepiness, or suspected sleep apnea.
Cardiology: recurrent palpitations, irregular-rhythm notifications, fainting, unexplained exercise intolerance, or known heart disease.
Pharmacist or prescribing clinician: a new drug, dose, supplement, or timing change followed by altered sleep, pulse, or HRV.
Medications and Substances That May Change the Picture
Many substances can alter heart rate, HRV, alertness, or sleep architecture. Examples include beta-blockers and other heart medicines, some antidepressants, stimulants, decongestants, steroids, thyroid medication, sedating antihistamines, sleep medicines, pain medicines, nicotine, cannabis, and alcohol; FDA medication-safety guidance urges older adults to review dose, timing, interactions, and recent prescription changes.
The direction of change is not always predictable, and the effect of a drug on a wearable metric is not the same as its clinical benefit or harm. A medication that lowers heart rate may change HRV readings without being inappropriate. A sedative may increase recorded sleep time while worsening breathing in a susceptible person.
Do not stop a prescribed medicine because an app score changed. Ask the prescribing clinician or pharmacist to review the medication, dose, timing, interactions, and recent changes. For older adults, this review is especially valuable because multiple medications can combine to affect balance, breathing, nighttime urination, and alertness.
Solutions That Support Both Recovery and Sleep
National Institute on Aging sleep guidance supports gradual and repeatable habits for older adults, including the following practical improvements.
Keep a Stable Sleep Opportunity
Set a regular wake time and allow enough time in bed for your sleep need. Avoid forcing an excessively early bedtime when you are not sleepy, which can increase time awake in bed. If insomnia persists, cognitive behavioral therapy for insomnia is the best-established non-drug treatment and can be delivered in person or through validated programs. For additional routine-building ideas, read how to sleep straight through the night while remembering that uninterrupted eight-hour sleep is not realistic for everyone.
Build Daytime Signals for Nighttime Sleep
Morning light helps anchor circadian timing. Regular aerobic activity and age-appropriate resistance training can support cardiovascular health, function, and sleep, but vigorous exercise may temporarily lower HRV when recovery is inadequate. Increase gradually and follow medical guidance if you have cardiovascular, pulmonary, or mobility limitations (CDC guidance recommends age-appropriate aerobic, strength, and balance activity for adults 65 and older).
Address the Disruptor, Not Merely the Score
Treat pain appropriately, discuss frequent urination, manage reflux, and evaluate persistent coughing or breathing difficulty. If snoring and gasping are present, do not rely only on sleep hygiene; request apnea screening. If worry about the device keeps you awake, hide the score for a week or ask a family member to help review only the weekly trend. Sleep position can also affect comfort, reflux, and breathing, as discussed in sleeping on the left side after 60.
Use Alcohol Cautiously
Alcohol can make a person sleepy initially yet fragment sleep later, suppress or shift sleep stages, worsen snoring and apnea, raise nighttime heart rate, and reduce recovery signals. A direct experiment—several alcohol-free nights under similar conditions—may be more informative than guessing.
Protect Hydration and Nutrition
Dehydration, inadequate intake during illness, and heavy late meals can affect sleep and heart-rate patterns. Aim for regular meals and daytime fluids appropriate to your medical conditions. People with heart failure, kidney disease, or prescribed fluid restrictions should follow their clinician’s plan rather than generic hydration advice; MedlinePlus identifies dark urine, dizziness, confusion, and reduced urination as dehydration warning signs. For a broader recovery framework, see Internal Terrain After 60 on hydration, nutrition, sleep, movement, and stress regulation.
What Not to Do With Low Smartwatch Scores
Do not diagnose heart disease or sleep apnea from HRV or deep-sleep minutes alone; clinical orthosomnia research shows that fixation on tracker scores can itself worsen sleep anxiety. Do not chase a universal HRV target found on social media. Do not compare values calculated by different devices as if they use the same method. Do not take unreviewed sleep supplements to improve an app score. Do not stop heart, blood-pressure, thyroid, psychiatric, or sleep medication without medical advice. Do not ignore symptoms because yesterday’s wearable score looked normal. Do not lose sleep trying to achieve “perfect” sleep data.
Your Personal Decision Card
Clinical orthosomnia research recommends using tracker data to guide questions rather than self-diagnosis, so complete these sentences and save them in your phone:
My usual nighttime HRV range: ________
My typical resting heart rate: ________
My current change began on: ________
Possible triggers: illness / stress / alcohol / exercise / pain / travel / medication / other: ________
Symptoms I have noticed: ________
My action: observe 7–14 days / contact clinician / urgent care / call 911
This small exercise turns an alarming color-coded score into a clear decision.
FAQs: Smartwatch HRV and Sleep Tracking Over 60
There is no single dangerous HRV number for every adult over 60. Devices use different sensors, time windows, and calculations. A persistent drop from your own baseline matters more than comparison with a population chart. Symptoms such as chest pain, fainting, severe breathlessness, or neurologic changes determine urgency. Discuss a sustained unexplained decline with your clinician.
Lower average HRV can be normal with aging, but a sudden personal decline is not automatically normal. Fitness, disease, medication, sleep, stress, and measurement method all contribute. Aging can explain a lower average compared with younger people; it does not automatically explain a sudden personal decline.
There is no universal deep-sleep-minute requirement for every 60-year-old. Deep sleep tends to decrease and become more fragmented with age. Because consumer devices estimate rather than directly measure sleep stages, focus on consistent sleep opportunity, daytime function, and trends.
A smartwatch estimates deep sleep; it does not clinically measure it. Studies show better performance for detecting sleep than for identifying individual stages. Treat deep-sleep minutes as an approximate trend, not a precise clinical measurement.
A sudden overnight HRV drop commonly reflects a temporary stressor or sensor problem. Check how you feel, review the previous day, ensure good device contact, and observe the next few nights. Seek care sooner if symptoms are present.
Sleep apnea can lower recovery signals and fragment deep sleep. A wearable may show poor sleep, oxygen variation, or unusual HRV, but it cannot confirm the diagnosis. Loud snoring, witnessed pauses, gasping, morning headaches, resistant hypertension, or daytime sleepiness should prompt formal screening. If you already use positive-airway-pressure therapy, the guide to CPAP dry mouth in older adults offers practical troubleshooting without recommending that you stop treatment.
HRV alone cannot diagnose atrial fibrillation. An irregular rhythm may change variability measurements, but confirmation requires an ECG or clinical rhythm monitor. Repeated irregular-rhythm alerts should be reviewed by a clinician. Seek urgent help if palpitations occur with fainting, chest pain, severe breathlessness, weakness, or stroke symptoms.
One night of zero displayed deep sleep is often a classification error. Repeat the measurement and consider how you feel. If the pattern repeats with unrefreshing sleep, major daytime sleepiness, snoring, gasping, or other symptoms, discuss it with a clinician rather than assuming you literally had no deep sleep.
There is no fixed number of low-HRV nights that requires a doctor call. If you feel well and have a plausible temporary trigger, observing a standardized 7- to 14-day trend is reasonable. Contact a clinician earlier if the decline is large, unexplained, associated with an increasing resting heart rate, or accompanied by fatigue, palpitations, breathlessness, or reduced exercise tolerance.
Dehydration can contribute to a lower nighttime recovery signal. Restore fluids appropriately, but follow medical restrictions if you have heart or kidney disease. Persistent abnormal readings or symptoms require more than hydration alone.
Alcohol commonly worsens sleep quality and recovery metrics. Many people see poorer recovery metrics after drinking. Several alcohol-free nights provide a useful personal comparison, but persistent symptoms still warrant assessment.
A demanding workout can temporarily lower next-morning HRV. This can happen especially if the training load increased suddenly or sleep and nutrition were inadequate. Reduce intensity briefly and watch for recovery. Chest discomfort, unusual shortness of breath, fainting, or a sustained decline in capacity should not be dismissed as training fatigue.
Medications can change HRV, pulse, breathing, alertness, and sleep structure. Heart medicines, antidepressants, stimulants, decongestants, steroids, thyroid drugs, sedatives, antihistamines, and pain medicines may influence pulse, autonomic activity, alertness, breathing, or sleep structure. Do not stop prescriptions based on a wearable.
Symptoms and daily function matter more immediately than either wearable score. Trends can add context and help identify patterns. A low score with no symptoms may justify observation; severe symptoms with a normal score still require care.
Check first for emergency symptoms. If none are present, make sure the device fits correctly, avoid alcohol and a heavy late meal, follow your normal medication plan, use a calm wind-down routine, and allow adequate sleep time. Record how you feel in the morning. Do not attempt extreme exercise, supplements, or medication changes to force a better score.
The Bottom Line on Senior Wearable Health Tracking
Low HRV and poor deep sleep after 60 can be a harmless combination of normal aging, temporary stress, and imperfect wearable estimation. They can also be early clues that the body is dealing with illness, inadequate recovery, medication effects, sleep apnea, or a cardiovascular problem. The numbers become more meaningful when they are persistent, different from your personal baseline, and accompanied by symptoms.
Use the device for what it does best: spotting patterns. Verify the quality of the reading, examine a consistent trend, listen to symptoms, and seek the appropriate level of care. The goal is not to produce a perfect green score every morning. It is to sleep and function well, recognize genuine warning signs, and act before a treatable problem is overlooked.
Authoritative U.S. Resources
Use these sources to verify wearable limitations, sleep-disorder pathways, cardiovascular warning signs, medication safety, and healthy-aging recommendations.
- National Institute on Aging – Sleep and Older Adults
- NHLBI – Sleep Apnea Symptoms and Diagnosis
- American Heart Association – Atrial Fibrillation Symptoms
- American Heart Association – Heart-Attack Warning Signs
- FDA – Medication Safety Tips for Older Adults
- CDC – Physical Activity Recommendations for Adults 65+
- MedlinePlus – Dehydration in Older Adults
- Peer-Reviewed Validation of Consumer Sleep Wearables
Medical note: This article provides general education for a U.S. audience and is not a diagnosis or a substitute for care from a licensed healthcare professional. Wearable metrics differ by device and are not independently sufficient to diagnose heart or sleep disorders. Call 911 for emergency symptoms.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.