In the final stage of life, the body naturally slows: appetite and thirst fade, sleep stretches longer, and breathing patterns may change. Comfort measures—gentle mouth care, calm lighting, soft repositioning, and unhurried sips—often help. If noisy or irregular breathing appears, it’s usually not painful; simple position changes can ease it. Palliative or hospice teams focus on comfort, symptom relief, and support for you and your family.

Understanding what is happening in the final stage of life can transform what feels frightening and unknown into something that is, at its core, a natural and often peaceful process. For both the person approaching the end of their life and for those who love them, knowledge is one of the most compassionate gifts available. The physical changes described in this article follow a well-understood trajectory that hospice nurses, palliative care physicians, and end-of-life researchers have documented over decades. They are not signs that something has gone wrong—they are signs that the body is moving through its final transition with its own wisdom. The role of caregivers, family members, and healthcare teams during this time is not to reverse what cannot be reversed, but to make the journey as comfortable, dignified, and surrounded by love as possible.
Table of Contents
The body’s natural slowdown
Appetite and thirst
Near life’s end, the body typically needs less fuel. Many people eat only a few bites, favor soft foods, or prefer moistening the mouth over drinking. Care teams often focus on comfort (moist lips, ice chips, favorite flavors in small amounts) rather than pushing full meals.
The decrease in appetite and thirst during the final stage of life is one of the most misunderstood and emotionally difficult changes for families to witness. It can feel like a loved one is “giving up” or “not being taken care of,” but research in palliative medicine tells a different story. The body’s metabolic needs genuinely decrease as organ function winds down, and the sensation of hunger is often absent. Hospice nurses and palliative physicians consistently report that patients who stop eating and drinking do not generally suffer from hunger or thirst in the way a healthy person would—the body’s natural chemistry during this stage, including the release of endorphins and the shift in ketone metabolism, appears to provide a form of natural comfort. Forcing food or fluids at this stage can actually cause distress, including nausea, bloating, and fluid accumulation in the lungs. The most compassionate approach is often to offer small amounts of a favorite food or drink as a gesture of love and connection—not as nutrition—and to keep the lips and mouth gently moistened. This is one area where hospice guidance is invaluable: their team can reassure families that honoring the body’s signals is an act of love, not neglect.
More sleep, less energy
Longer sleep and low energy are common. You might feel best dozing, listening to a familiar voice, or enjoying quiet music; brief wakeful moments are often enough.
Increasing sleepiness in the final stage of life reflects a gradual withdrawal of the body’s energy inward, as resources are conserved for essential functions. This is a fundamentally different kind of sleep than ordinary tiredness—it is deeper, more sustained, and often accompanied by a reduced response to external stimulation. For families, this can be heartbreaking; the person they love seems to be “drifting away.” But hearing remains one of the last senses to fade, and researchers in consciousness and anesthesiology believe that even deeply unconscious patients may be aware of voices and sounds around them. Speaking gently and calmly to a sleeping loved one—sharing memories, expressing love, reading aloud from a favorite book, or simply sitting in quiet presence—is never wasted. Many hospice teams encourage family members to continue speaking, singing, or playing meaningful music even when the person appears deeply asleep. Brief wakeful periods become precious windows; keep them calm, unhurried, and free of difficult decisions or distressing conversations.
Breathing changes
Breathing can grow irregular—sometimes with cycles of deep breaths, shallow breaths, then pauses (Cheyne-Stokes). A gentle turn to one side or elevating the head can reduce “noisy” or rattly breathing; it usually bothers family more than the person resting.
Cheyne-Stokes respiration—named for the two physicians who described it in the 19th century—is a distinct breathing pattern characterized by gradually deepening and then diminishing breaths, followed by a brief period with no breathing at all, before the cycle repeats. It occurs because the brain centers that regulate breathing become less responsive to carbon dioxide as circulation slows. It is not a sign of pain or distress; clinical assessments of patients experiencing Cheyne-Stokes consistently show no behavioral indicators of suffering. The “death rattle”—a term hospice teams gently discourage because of its frightening connotations—is the sound of air moving past accumulated secretions in the throat and airways that the person no longer has the muscular strength to clear. It is generally not painful; the relaxed state of the throat tissues means the sound is more disturbing to observers than to the patient. Repositioning the person slightly—raising the head of the bed by 30 degrees, or turning to one side—often reduces the sound significantly. If it persists and causes visible distress, hospice clinicians have medications that can help manage it.
Thinking and awareness
Periods of confusion, vivid dreams, or brief agitation can occur. A calm voice, soft lighting, and simple reassurance often help. Tell your clinician about new restlessness—they can suggest comfort options.
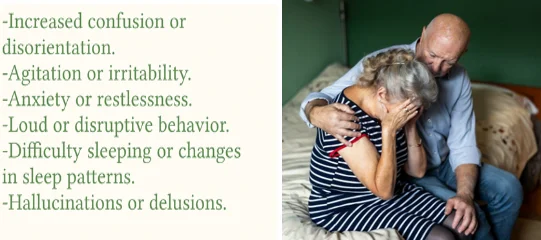
The phenomenon of terminal restlessness or agitation—called “terminal delirium” in the clinical literature—affects roughly 25 to 85% of dying patients in their final days and hours. It can be deeply upsetting to witness, involving picking at bedclothes, attempting to get out of bed, mumbling, or calling out. Its causes are multiple and often treatable: uncontrolled pain, a full bladder, constipation, medication side effects, or profound metabolic changes in the brain. Before assuming agitation is an inevitable or untreatable part of dying, always inform the hospice or palliative team—because many causes are reversible with gentle interventions, and medications exist that can provide effective relief without hastening death. Some people in the final stage also experience what clinicians call “terminal lucidity”—a sudden, unexpected period of clarity and coherence after days or weeks of confusion, during which they may have meaningful conversations, recognize loved ones, or express their feelings. This phenomenon is well-documented and treasured by families who experience it. Receive it as a gift, and do not be confused if it is followed by a return to the previous state—it does not mean recovery is happening.
Comfort first: simple things that help
- Mouth care: frequent sips, swabs, or lip balm ease dry mouth when drinking is hard.
- Positioning: small pillow shifts (under knees/side), head elevation, and unhurried turns reduce pressure and ease breathing.
- Quiet routine: dim light, favorite sounds, and short visits conserve energy and ease end-of-life restlessness.
- Care team support: palliative or hospice clinicians can adjust meds, teach gentle care steps, and support family questions.




Comfort care in the final stage of life is both an art and a science, and the specific interventions listed above are among the most evidence-based tools available for ensuring dignity and peace. Oral care deserves special emphasis: as swallowing becomes difficult and mouth breathing increases, the mouth becomes dry, sticky, and uncomfortable. Small oral foam swabs moistened with water, or a soft toothbrush dipped in cool water, can provide significant relief. Apply a gentle lip balm—unflavored, or a flavor the person likes—every hour or two to prevent painful cracking. Repositioning is equally important: as mobility decreases, pressure injuries (bedsores) can develop within hours on bony prominences like heels, hips, and the tailbone. Small, gentle turns every two hours—or more frequently if needed—are standard hospice nursing practice. You do not need to roll the person completely; even a small shift of position, supported by a foam wedge or folded blanket, can relieve pressure meaningfully. The quiet routine matters too: research on the neuroscience of dying suggests that familiar sensory environments—soft light, known voices, beloved music played at low volume—create a sense of safety that reduces agitation and supports a more peaceful transition.
Care options in the U.S.
Palliative care can begin at any stage of serious illness and focuses on comfort alongside other treatments.
Hospice care centers on comfort when treatments no longer help or are no longer desired. Ask your clinician about local programs and home-based options.
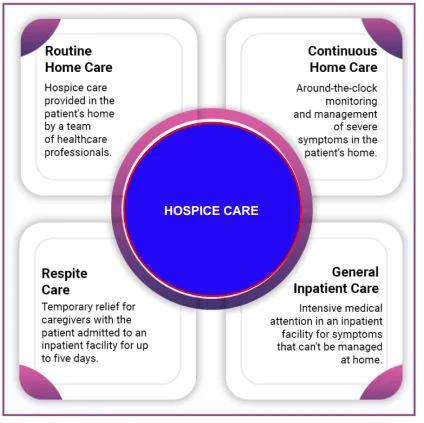
One of the most common and heartbreaking misunderstandings about end-of-life care in the U.S. is that hospice is “giving up.” In reality, decades of research consistently shows that patients enrolled in hospice programs often live as long as—and sometimes longer than—similar patients who continue aggressive curative treatment, while experiencing significantly better quality of life, less pain, and fewer hospitalizations. A landmark 2010 study published in the New England Journal of Medicine found that lung cancer patients who received early palliative care lived nearly three months longer on average than those receiving standard care alone. To qualify for Medicare hospice benefits, a physician must certify that if the illness runs its normal course, the patient is expected to live six months or less—but enrollment does not mean giving up the possibility of more time. Hospice teams include physicians, nurses, social workers, chaplains, and home health aides who make regular visits, provide all necessary medications and equipment, and offer 24/7 phone support. Home hospice—allowing a person to die in their own home—is available to the vast majority of patients and is the most commonly chosen option when people are informed of what it entails. Palliative care, meanwhile, is available at any stage of a serious illness and can be provided alongside curative treatments by a specialized team focused on comfort, communication, and quality of life.
Gentle language, clear signs (for seniors themselves)
- Body slowing down: smaller appetite, longer naps, lighter conversations.
- Breathing looks different: uneven rhythm, brief pauses; often not painful.
- Comfort over calories: moist mouth, favorite tastes, and rest beat “finishing a plate.”


For the senior reading this themselves, these words are offered with deep respect and care. What is happening in your body is not failure—it is completion. The changes you may be noticing or anticipating are the same ones that have accompanied the end of every human life before yours, and they are manageable and usually peaceful when supported well. The most important things you can do right now are to tell the people around you what you want—where you want to be, who you want present, what music matters to you, what you need said, what you need forgiven, what you want remembered. These conversations, however difficult they feel, are among the most profound gifts a person can give. If you have not already spoken with a palliative care team or a hospice program, ask your physician today. You deserve a team of people whose sole focus is your comfort and dignity. And know that what those who love you want most—more than anything—is for you to be at peace.
Discover-friendly Q&A (quick answers)
1) What does “final stage of life” usually feel like?
Quieter days, more sleep, and a fading appetite; comfort—rather than fixing every symptom—is the priority.
Most people who are actively dying describe the experience—during their lucid moments—as a peaceful withdrawal from the external world rather than a painful confrontation with it. The term “actively dying” is used by hospice clinicians to describe the final hours to days of life, distinguished from the broader “end-of-life” period that may span weeks or months. During the active dying phase, the body’s focus turns entirely inward, and many patients appear calm and restful even to those who are anxious about what they are witnessing.
2) Why don’t I feel hungry or thirsty?
Your body needs less energy now; mouth care and small sips can be more soothing than full meals.
3) My breathing pauses—should I worry?
Brief pauses and changing patterns (Cheyne-Stokes) can be part of this stage; turning on your side or raising the head often helps.
4) What is the “rattle” sound?
Air moving over pooled secretions; it’s usually not distressing to the resting person and often eases with repositioning.
5) Why am I sleeping so much?
Energy wanes as systems slow; more sleep is normal and protective.
6) How can my family keep me comfortable?
Soft lighting, calm conversation, mouth care, gentle turns, and unhurried time together.
7) Is palliative care the same as hospice?
No. Palliative care can start anytime to ease symptoms; hospice focuses on comfort near life’s end.
Palliative care is a specialty layer of medical care focused on relief from pain, stress, and other symptoms of serious illness. It is appropriate at any age and at any stage of a disease, and can be provided alongside curative treatment. Hospice is a specific type of palliative care for people who are no longer pursuing curative treatment and have an estimated prognosis of six months or less if the disease runs its normal course. Both represent deeply compassionate, patient-centered approaches to serious illness.
8) Are appetite stimulants or IV fluids helpful now?
Sometimes they’re not beneficial and can add discomfort; discuss pros/cons with your clinician or hospice team.
9) I feel restless or confused at night—what helps?
A quiet room, familiar voices, and routine; clinicians can offer safe, low-dose options if needed.
10) When should my family call the nurse?
Any sudden pain, new distress, falls, or questions about medicines—comfort teams want to hear from you.
11) Where can we learn more right now?
The National Institute on Aging’s end-of-life pages offer clear, practical guidance.
12) What if I want to stay at home?
Hospice and palliative programs can often arrange home-based support, equipment, and 24/7 advice.
A calm end-of-day checklist
- Soft lamp or night-light on; room quiet and slightly cool.
- Mouth moistened; favorite balm on lips.
- Pillows placed for easy breathing (head elevated, side-lying if helpful).
- Short visit or music you enjoy; phone silenced except for essentials.
- Questions listed for the next nurse or clinician call.
This checklist is deliberately simple—because the final stage of life calls for simplicity, not complexity. It calls for presence over procedure. The five items above represent what hospice nurses identify as the most consistently soothing end-of-day rituals for both the dying person and the family members caring for them. The act of going through a gentle, predictable evening routine communicates safety and love in ways that words sometimes cannot. If you are a caregiver reading this, know that the comfort you bring through these quiet acts is profound. You do not need to say the right thing, fix anything, or know all the answers. Your steady, loving presence—the warmth of a hand held, the soft sound of a familiar voice, the glow of a gentle lamp in a quiet room—is everything.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.