DNA Tests After 60: Diet and Medication Response
Adults over 60 usually benefit most from the narrowest DNA test that can change a real decision. Pharmacogenomic testing may help with selected medication choices; focused gene panels may clarify a strong family history; WES or WGS is generally reserved for unresolved cases. DNA nutrition results can suggest tendencies, not prescribe a perfect diet. Confirm important findings and review medication-related results with a clinician before acting.
Executive Summary
After 60, DNA testing becomes more practical when it answers a real clinical question. The central issue is not “Should I get a DNA test?” but “Which test changes a real decision?” A targeted pharmacogenomic panel may help if you are choosing or reacting badly to a medication. A focused single-gene or panel test may help if your family history points toward a specific inherited condition. Whole-exome or whole-genome sequencing is usually a later-step test when single-gene or panel testing has not explained the problem or when the genetic cause is unclear. MedlinePlus notes that broader sequencing is typically used when narrower testing has not provided a diagnosis or when the suspected cause remains unclear.
For pharmacogenomics and medication response, the evidence is strongest when a specific drug–gene pair already matters in clinical care. The FDA’s pharmacogenetic associations table includes examples relevant to older adults: citalopram with CYP2C19, clopidogrel with CYP2C19, and codeine with CYP2D6. In these cases, genotype can affect drug concentration, effectiveness, or toxicity risk. That is why pharmacogenomics is often more actionable than broad consumer wellness genomics for adults over 60. For a closer look at how a low blood sugar warning sign or medication response question might come up in daily life, see our guide on warning signs your blood sugar is too high after 60.
For diet, expectations should stay realistic. Consumer DNA nutrition tests can sometimes be useful for narrow issues such as known intolerance-related pathways, nutritionally relevant inherited conditions, or caffeine-handling tendencies. But broad claims that a cheek-swab alone can identify your best long-term weight-loss diet, ideal macronutrient split, or personalized supplement stack are much less established clinically than the best-used pharmacogenomic applications. That conclusion is an inference from the current strength of FDA-recognized drug–gene guidance, the more limited clinical use cases for broad nutrition DNA testing, and the fact that most genetic test results require interpretation in context.
Whole-genome and whole-exome sequencing can reveal more information than you asked for. MedlinePlus explains that these broader tests may uncover secondary findings unrelated to the original reason for testing, including findings tied to cancer or cardiovascular risk. Patients can usually choose whether to receive these secondary findings. That benefit can be valuable, but it also creates more follow-up testing, more decision-making, and more anxiety if results are unclear or unexpected. For more on cardiovascular risk findings specifically, see our guide on preventing clogged arteries.
Cost, coverage, privacy, and family impact matter more after 60 than many shoppers first realize. MedlinePlus states that genetic testing can cost from under $100 to more than $2,000, depending on complexity, and results may take days to weeks. Insurance often covers testing when it is recommended by a doctor, but policies vary. Genomic information can also matter beyond you alone because positive results may affect relatives, and U.S. genetic-discrimination protections are meaningful but incomplete: Genome.gov explains that GINA protects against many health-insurance and employment uses of genetic information, but it does not cover life insurance, disability insurance, or long-term care insurance.
Assumptions used in this article: your exact budget is not specified, your access to a genetic counselor is not specified, and your medication list is not specified. The recommendations below are therefore structured around common decision pathways for U.S. adults over 60 rather than a single disease scenario.
What DNA Tests After 60 Mean
A DNA test after 60 is best understood as a decision support tool. It does not diagnose most common chronic diseases by itself. Instead, it can help answer one of four questions: Do I carry a variant linked to a known inherited condition? Could a gene help explain a medication failure or side effect? Should I consider broader sequencing because narrower testing did not explain the problem? Does my family need to know this result?
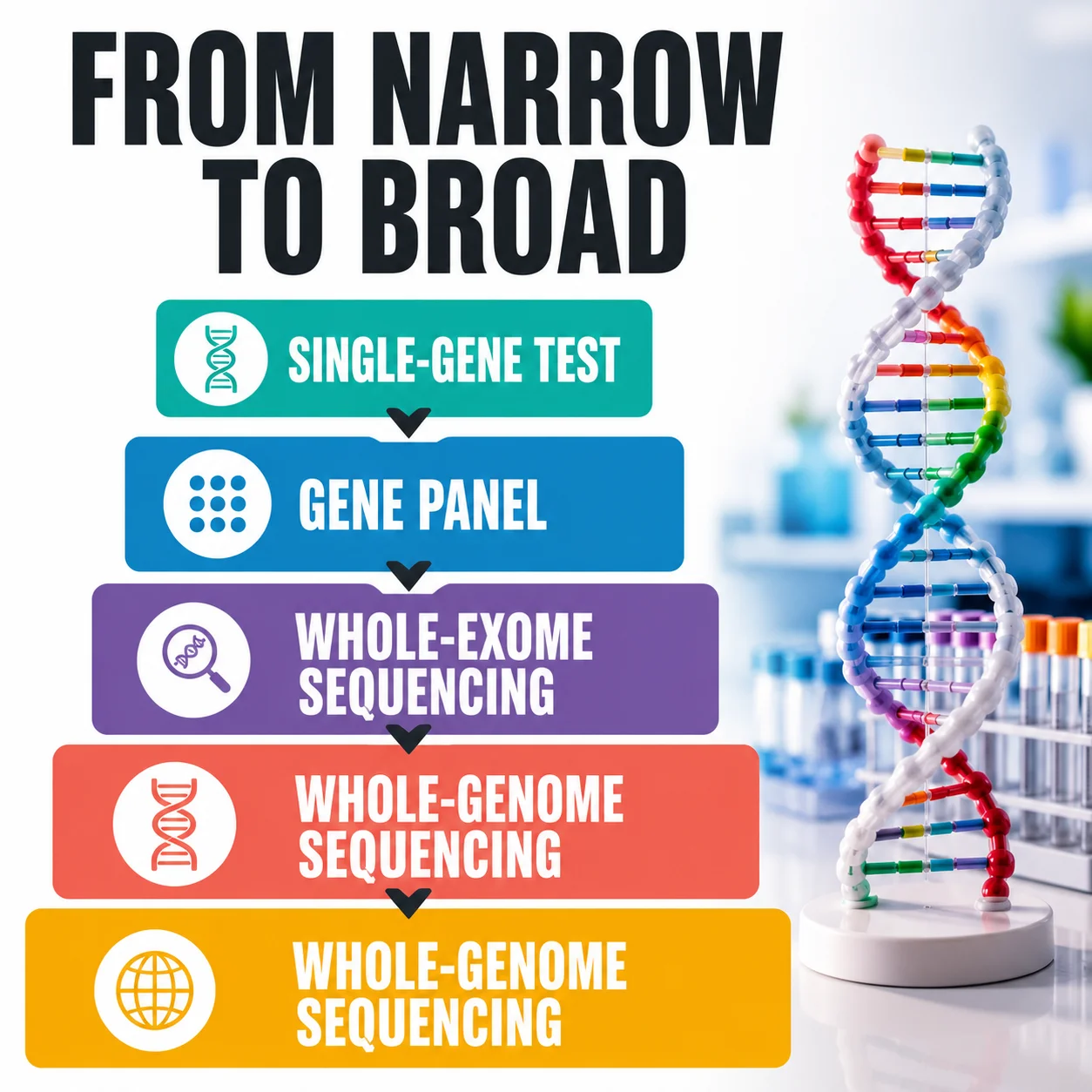
MedlinePlus divides testing into several categories: targeted single-variant testing, single-gene testing, gene panels, whole-exome or whole-genome sequencing, chromosomal testing, gene-expression testing, and biochemical testing. Direct-to-consumer tests often analyze selected variants rather than comprehensively reading every relevant variant in a gene. That distinction matters. A consumer kit may be good at giving a broad signal, but a clinician often needs a more focused or more complete test to make medical decisions.
Results also come in more than one flavor. A result can be positive, negative, or uninformative. MedlinePlus notes that a positive result may confirm a diagnosis, indicate carrier status, or identify an increased risk, but it usually cannot predict the exact severity or timetable of disease. A negative result does not always rule something out because tests do not detect every possible disease-causing change. And a variant of uncertain significance can leave you in the frustrating middle ground where the lab found something, but science cannot yet say whether it is clinically important.
For a lay reader, the simplest way to think about DNA testing after 60 is this: your genes are not your fate, but they can change the probability landscape. Sometimes they change it a little. Sometimes they change it enough to alter the medication, screening plan, or advice given to relatives. The mistake is expecting every result to deliver a dramatic, one-step answer.
| Test Category | What It Looks At | Best Use After 60 | Main Upside | Main Limit |
|---|---|---|---|---|
| Direct-to-consumer selected-variant test | A chosen set of variants | Early curiosity, ancestry, limited health screening | Easy access | Often not comprehensive enough for major medical decisions |
| Single-gene test | One gene in depth | Strong suspicion of one inherited condition | Precise when the clue is strong | Too narrow if the diagnosis is unclear |
| Gene panel | Multiple related genes | Medication response, hereditary cancer clues, unexplained but focused syndromes | Good balance of scope and interpretability | Can still return uncertain findings |
| Whole-exome sequencing | Most protein-coding DNA | When panel testing is unrevealing and the cause is unclear | Broader diagnostic reach | More secondary findings and interpretation burden |
| Whole-genome sequencing | Nearly all DNA | Complex unresolved cases, broader variant search | Widest scope | Highest interpretation complexity and potential follow-up burden |
This comparison is based on MedlinePlus explanations of test types and result interpretation.
Which Test Fits Which Goal
Before comparing brands, write down the decision you want the result to support. Useful questions include whether a current medicine may be affected by a known drug–gene relationship, whether a strong family pattern warrants targeted clinical testing, or whether a persistent food-related symptom deserves conventional evaluation before genetics is considered. Also note what you would do differently if the result were positive, negative, or uncertain. If none of the possible outcomes would change care, screening, or a practical habit, testing may add cost and anxiety without adding much value.
Prepare a one-page information sheet before speaking with a clinician or counselor. Include all prescriptions, over-the-counter medicines, supplements, prior adverse drug reactions, major diagnoses, and any relevant laboratory results. Add a three-generation family history when possible, noting the condition and approximate age at diagnosis rather than writing only “cancer” or “heart disease.” This preparation helps distinguish a medication-response question from an inherited-disease question and makes it easier to choose between a single-gene test, a focused panel, or broader sequencing.
The right DNA test depends on the job you need it to do. If your question is, “Why did I react badly to this medicine?” then a pharmacogenomic panel is usually the better first move. If your question is, “Several relatives had the same cancer,” then a hereditary-risk panel is the better first move. If your question is, “We still do not know why this condition is happening after focused testing,” then exome or genome sequencing becomes more reasonable.
The broadest test is not automatically the smartest test. MedlinePlus specifically says that whole-exome or whole-genome sequencing is typically used when single-gene or panel testing has not provided a diagnosis or when the suspected cause is unclear. In plain English, broader sequencing often belongs later in the process, not first. That sequence can save money, reduce confusion, and lower the chance of unrelated surprises.
Cost and insurance also push test choice. MedlinePlus says overall genetic-testing costs range from under $100 to more than $2,000, and insurance often covers testing when a doctor recommends it, though policies differ. A practical rule is to start with the narrowest test that can actually answer the question in front of you. That is the version most likely to stay clinically clear and financially reasonable.
| Your Main Goal | Best Starting Test | Why This Is Usually the Right Starting Point | Cost Direction |
|---|---|---|---|
| Learn about ancestry or broad personal-interest traits | Direct-to-consumer selected-variant test | Good for curiosity, not ideal for medication changes | Lower end |
| Check a suspected drug–gene interaction | Pharmacogenomic panel | Action links to a real prescription decision | Lower-to-middle range |
| Investigate a strong family-history clue | Focused single-gene or hereditary-risk panel | Matches the family pattern directly | Middle range |
| Solve an unresolved medical puzzle after negative focused testing | Whole-exome or whole-genome sequencing | Broader search when narrower testing failed | Upper range |
| Clarify a previously unclear result | Confirmatory clinical testing with counseling | Reduces overreaction to uncertain or incomplete data | Varies |
The cost-direction column is an editorial interpretation of MedlinePlus’s official overall range and its description that complexity increases cost. The exact bill depends on laboratory scope, ordering pathway, and insurance status.
What Diet and Medication Response Results Can Really Do
Pharmacogenomics: The Most Actionable Use After 60
Here is the blunt truth: medication-response testing is usually where DNA becomes most concrete after 60. The FDA’s pharmacogenetic associations table shows examples where genotype changes recommended dosing, risk interpretation, or drug choice. For instance, the FDA notes that citalopram in CYP2C19 poor metabolizers can produce higher concentrations and greater QT-prolongation risk, with a maximum recommended dose of 20 mg. The FDA also notes that clopidogrel in CYP2C19 intermediate or poor metabolizers can lead to lower active-metabolite levels and lower antiplatelet response, and that another platelet P2Y12 inhibitor should be considered. For codeine, the FDA notes higher toxicity risk in CYP2D6 ultrarapid metabolizers and reduced efficacy in CYP2D6 poor metabolizers.
The clopidogrel example shows why DNA can matter in everyday senior care. NCBI’s clopidogrel and CYP2C19 summary explains that clopidogrel is a prodrug that must be activated by CYP2C19. Poor metabolizers cannot activate it well and may have a reduced antiplatelet effect. The same review also notes that co-medications can change effective CYP2C19 activity, which means genes are important but not the whole story. In real life, the clinician still has to consider the full medication list, other illnesses, and whether another drug may be safer or more effective.
That last point is essential for medication safety after 60: DNA results do not replace clinical pharmacology. They add one layer to it. A DNA result can tell you that a pathway is slower, faster, or altered. It cannot by itself account for kidney decline, liver disease, frailty, dehydration, food–drug interactions, or the effect of another medicine blocking the same enzyme.
Why Medication Context Matters More With Age
A pharmacogenomic result is only one part of medication review. After 60, the same drug response may also be influenced by kidney or liver function, body composition, dose, adherence, dehydration, and interactions among several medicines. These factors can change over time even though inherited DNA does not. That is why an older report should be interpreted against the current medication list and current clinical measurements rather than treated as a permanent dosing instruction. A useful result identifies a question for the prescriber or pharmacist; it does not authorize a patient to stop, start, substitute, or change a dose independently.
When ordering a medication-response test, ask exactly which genes and variants are included, whether the laboratory uses a clinical confirmation process, and whether the report connects results to a recognized prescribing guideline or regulatory label. Coverage varies among panels, so a report labeled “pharmacogenomics” may not address the medicine that prompted the test. Bring the complete laboratory report—not only a colored dashboard or app summary—to the appointment. The clinician needs the genotype, the laboratory method, the interpretation, and the report limitations to decide whether the finding is relevant. For related medication decision-making, see our guide on questions to ask your doctor before starting a new medication after 60.
DNA Diet Results: Caffeine, Lactose and Nutrient Pathways
Diet-response testing is more mixed. A narrow nutrition-related genetic result can be genuinely useful when it maps onto a real behavior or symptom. But most older adults should view large commercial DNA diet reports as hypothesis generators, not verdicts. If the report says you may handle caffeine slowly, that may support earlier caffeine cutoffs if you already notice palpitations or poor sleep. If a report says you may have lactose-related issues, it may help explain symptoms. But DNA does not erase the need to look at blood sugar, cholesterol, weight trend, appetite, bowel symptoms, kidney function, strength, sleep, and actual food intake.
The most understandable nutrigenomic examples are narrow and testable. CYP1A2 variants may contribute to differences in caffeine metabolism, while the LCT/MCM6 region is associated with lactase persistence and lactose tolerance. These relationships can add context, but symptoms are also shaped by dose, sleep, medicines, anxiety, gut health, food pattern, and ancestry. A genetic tendency is not a diagnosis of intolerance, deficiency, or disease.
How to Judge a DNA Nutrition Recommendation
Judge each nutrition claim by asking three questions. First, does the test measure a clearly identified variant rather than a vague wellness score? Second, is the proposed action safe and sensible for an older adult with your diagnoses and medicines? Third, can the recommendation be checked against symptoms, dietary intake, or routine clinical testing? A modest change—such as adjusting caffeine timing while monitoring sleep—is easier to evaluate than a restrictive diet built from dozens of small genetic associations. Be especially cautious when a report recommends expensive supplements, eliminates major food groups, or implies that genetics overrides medical nutrition advice.
For nutrient-related findings, the next step is usually confirmation, not automatic supplementation. A genetic tendency does not prove that a deficiency is present today, and high-dose supplements can interact with medicines or create their own risks. Discuss the result with a clinician or registered dietitian who can consider food intake, symptoms, kidney function, and appropriate laboratory measurements. The most useful nutrition report should narrow a question and support a measurable trial; it should not convert a small statistical association into a lifelong rule.
Analytical Accuracy vs Clinical Usefulness
A laboratory can identify a tested variant accurately while the interpretation attached to that variant remains uncertain or only modestly useful. Analytical validity asks whether the laboratory measured the DNA change correctly. Clinical validity asks how strongly the change relates to an outcome. Clinical utility asks whether knowing it improves a real decision. The broader the wellness claim, the more important it is to separate these three questions.
| Result Type | Example | What It Can Change | What It Should Not Replace |
|---|---|---|---|
| Strong drug–gene signal | Clopidogrel + CYP2C19 | Choice of antiplatelet strategy | Cardiology judgment, bleeding-risk review |
| Drug concentration/toxicity signal | Citalopram + CYP2C19 | Dose ceiling and ECG-aware caution | Electrolyte review, QT-risk review, other drugs |
| Drug activation signal | Codeine + CYP2D6 | Avoidance or alternative pain control | Pain assessment, constipation/fall-risk planning |
| Narrow nutrition signal | Caffeine-handling or intolerance clue | Lifestyle trial with symptom tracking | Full nutrition assessment and routine labs |
| Broad wellness DNA summary | Mixed diet/supplement suggestions | Conversation starter | Evidence-based diet and chronic-disease care |
This table summarizes FDA-labeled drug–gene examples and MedlinePlus guidance on interpreting results and limitations.

When Whole-Genome Sequencing Helps and When It Does Not
Whole-Exome vs Whole-Genome Sequencing
Whole-genome sequencing sounds like the ultimate answer because it reads vastly more DNA. But broader is not automatically better. MedlinePlus states that whole-exome or whole-genome sequencing is typically used when single-gene or panel testing has not solved the case or when the suspected genetic cause is unclear. That means the best question for a shopper over 60 is not “Can I afford genome sequencing?” but “Am I at the stage where genome sequencing is justified?”
Whole-exome sequencing, or WES, focuses mainly on protein-coding regions. Whole-genome sequencing, or WGS, examines coding and non-coding regions more broadly. WGS produces more data, but more data does not automatically create more useful answers. Coverage, variant type, laboratory method, clinical question, and interpretation quality all affect what a test can find and whether a result is actionable.
Where WGS or WES can help is in complex unresolved cases. If there is a longstanding unexplained condition, unusual family pattern, or prior negative focused testing, broader sequencing may find a diagnosis that a smaller test missed. It can also identify clinically important secondary findings. MedlinePlus explains that broader sequencing can reveal variants unrelated to the original indication, such as variants tied to BRCA1 or LDLR, and that patients can opt out of receiving analysis for the ACMG secondary-finding gene list.
Where WGS does not shine is as a universal shortcut for healthy aging. It can generate more findings than your care team can immediately use. It can return uncertain results. It can start a chain of repeat testing, screening, and worry for findings that may never cause disease. MedlinePlus emphasizes that unexpected results may lead to additional costs and stress, even when the information is medically important.
Privacy, Secondary Findings and Genetic Counseling
Genome.gov explains that GINA blocks many health-insurance and employment uses of genetic information, and those protections extend across private health insurance, Medicare, Medicaid, and federal employee coverage. But it also states that GINA’s health-insurance protections do not cover life insurance, disability insurance, or long-term care insurance. For a reader over 60, that gap deserves real attention before buying broad sequencing just because it is available.
On cost, MedlinePlus gives the practical consumer frame: testing can cost under $100 to over $2,000, with complexity driving price. NHGRI’s sequencing-cost tracking shows that the raw technical cost of sequencing has fallen dramatically over time, but those figures do not include the full downstream costs of interpretation, counseling, confirmatory work, and follow-up management. In other words, the cheap part is increasingly the readout; the expensive part is deciding what the readout means for a real person.
Questions to Ask Before Broad Sequencing
Before WES or WGS, decide how much information you actually want returned. Ask whether the laboratory reports medically actionable secondary findings, carrier findings, uncertain variants, or adult-onset risks unrelated to the original question. Clarify whether you can opt in or out of categories, whether important findings require confirmation in a second sample, and whether reinterpretation is available as scientific knowledge changes. Also ask who can access the raw data, how long the sample is stored, whether data may be used for research, and how deletion requests are handled. These choices are easier to make before testing than after an unexpected result appears.
Family implications deserve the same advance planning. A result may explain your own health question while also suggesting that children, siblings, or other blood relatives could benefit from targeted evaluation. It can also reveal information that relatives did not expect or want to know. A genetic counselor can help separate a result that requires prompt communication from one that remains uncertain, prepare a plain-language family letter, and identify which relatives should consider testing. Whenever possible, share the verified clinical finding rather than screenshots or raw-data interpretations from a consumer platform.
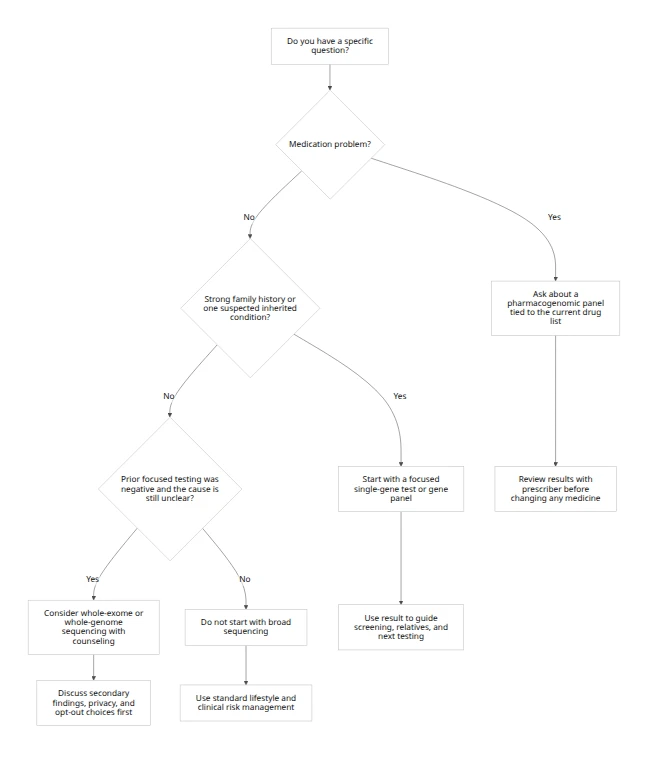
| Medication Question | Family-History Question | Unresolved Diagnosis |
|---|---|---|
| Start with a targeted pharmacogenomic panel | Start with a focused single-gene or hereditary-risk panel | Consider WES or WGS after narrower testing |
| Review with the prescriber or clinical pharmacist | Review with a genetics clinician or specialist | Review with a clinical genetics team |
Decision shortcut: begin with the narrowest test that can answer the question, then broaden only when the clinical problem remains unresolved.
How to Act on Results Safely
How to Interpret Increased Genetic Risk
The safest way to use a DNA result after 60 is to turn it into a small, documented action, not a dramatic self-directed overhaul. If the result concerns a medication, bring the report and your full medication list to the prescriber or pharmacist. If the result concerns inherited disease risk, write down the exact variant, the condition name, and which relatives may need the information. If the result is uncertain, do not build a treatment plan around it. MedlinePlus is clear that a VUS may not be disease-causing and that unclear results can remain uninformative.
An increased genetic risk is a probability compared with a reference group, not a prediction that an outcome will happen. Ask for the absolute risk as well as the relative change, how well the association applies to your ancestry and health history, and whether the result has been clinically confirmed. Family history, environment, age, current biomarkers, and preventive care can be more important than a single variant.
A practical action pathway looks like this: first, identify whether the result is about drug response, disease risk, or uncertainty. Second, ask what concrete decision the result changes this month. Third, check whether confirmatory or more focused clinical testing is needed. Fourth, decide what relatives should know. Fifth, document privacy choices, including research consent and whether you want the result stored in patient portals or shared more narrowly.
Older adults should also pause before using insurance if they are considering broad predictive testing with uncertain immediate medical value. MedlinePlus says many plans cover doctor-recommended testing, but people may still choose to pay out of pocket or use direct-to-consumer routes. Genome.gov’s explanation of GINA shows why some people think carefully about the timing of testing relative to long-term care, disability, or life-insurance decisions. This is not a reason to avoid needed testing; it is a reason to plan the order of operations.
| Result Pattern | Immediate Next Step | Best Person to Review It With | Common Mistake to Avoid |
|---|---|---|---|
| Actionable drug–gene result | Reconcile all prescriptions and supplements | Prescriber or clinical pharmacist | Changing the dose on your own |
| Positive hereditary-risk result | Confirm family history and screening plan | Genetics clinician or specialist | Assuming relatives do not need to know |
| Negative result but strong suspicion remains | Ask whether the test scope was broad enough | Ordering clinician | Treating negative as absolute |
| Variant of uncertain significance | Document and monitor reclassification | Genetics professional | Making major medical decisions from a VUS |
| Broad sequencing with secondary findings | Separate primary finding from incidental finding | Genetic counselor and relevant specialist | Letting incidental findings drive panic |
This action table summarizes MedlinePlus guidance on interpretation, limitations, and insurance planning, combined with Genome.gov’s explanation of legal protections and gaps.
Create a Results Follow-Up Plan
Store the final laboratory report with your medication and health records, and record the date, laboratory, ordering professional, and reason for testing. For a medication-related result, ask whether the information should be added to the electronic health record or pharmacy profile so it is visible during future prescribing. For inherited disease risk, document the recommended screening or referral rather than relying on memory. If the finding is uncertain, record what would trigger reinterpretation and who is responsible for requesting it. A clear follow-up plan prevents an important result from becoming an isolated PDF that no one uses.
Revisit the result when a relevant medicine is started, when a major diagnosis changes the clinical picture, or when the laboratory issues a revised interpretation. Do not repeatedly retest inherited variants simply because time has passed; the DNA is generally the same, although evidence and clinical guidance may evolve. The practical goal is continuity: one verified result, interpreted in the right context, communicated to the right professionals, and translated into a specific action only when the evidence supports it.
Frequently Asked Questions
Yes. A DNA diet test can be worth buying after 60 when it answers a narrow, real-life question, but it is usually not enough to build your whole nutrition plan by itself. Use it as one clue alongside symptoms, lab work, medical conditions, appetite, weight trend, and food quality.
Yes. Pharmacogenomic testing is usually more useful than a general wellness DNA kit after 60 when the goal is to improve medication safety or response. The strongest current clinical use cases are tied to specific drug–gene pairs that can affect dose, efficacy, or side effects.
No. A DNA test cannot reliably choose your best long-term weight-loss diet by itself. Diet success still depends heavily on calorie balance, protein intake, food quality, adherence, sleep, physical activity, medical conditions, and medications.
Sometimes. A DNA test can sometimes show that your body may process or activate a drug differently, but it usually cannot guarantee whether a drug will work perfectly for you. Genes are one part of prescribing, along with diagnosis, dose, kidney function, liver function, interactions, and other clinical factors.
No. You should not change your medicine based on a home DNA test without a clinician reviewing the result in the context of your full medication list and health status. A result may be incomplete, may need confirmation, or may be outweighed by other clinical factors.
No. Whole-genome sequencing and pharmacogenomic panels are not the same test and do not serve the same purpose. A pharmacogenomic panel is a targeted clinical tool for medication response, while whole-genome sequencing is a much broader search that may uncover unrelated findings.
No. A negative DNA result cannot rule out future drug side effects. Side effects can still happen because of age, dose, kidney function, drug interactions, dehydration, or non-genetic biology.
A variant of uncertain significance is a DNA change that has been found but cannot yet be confidently classified as harmful or harmless. It should usually prompt caution, not panic, and it should not automatically drive major treatment decisions.
No. DNA testing cannot replace cholesterol, A1c, kidney, or liver tests. DNA shows inherited tendency and some medication-response pathways, while routine clinical tests show what your body is doing right now.
Usually. Insurance often covers genetic testing after 60 when a doctor recommends it, but coverage rules vary widely by plan and by test type. It is smart to check benefits before testing unless the clinical need is urgent and the ordering team handles preauthorization.
Usually. Family members should often know about an important DNA result because a positive finding may have implications for blood relatives. The closer the inherited condition is to family risk, the more important this conversation becomes.
Yes. You should think seriously about privacy before ordering broad DNA testing, especially if the result is not medically urgent. U.S. law protects against some uses of genetic information, but protections do not fully extend to life insurance, disability insurance, or long-term care insurance.
A genetic counselor can help when a result is unclear, emotionally heavy, relevant to relatives, or likely to affect major screening or treatment decisions. Counseling is especially useful before whole-exome or whole-genome sequencing and after an unexpected positive result.
The best first DNA test for most adults over 60 is usually the narrowest test that answers the medical question in front of them. That often means a pharmacogenomic panel for medication response or a focused panel for a strong family-history clue rather than broad genome sequencing.
Yes. You can skip DNA testing and still improve your health after 60 through evidence-based habits, regular medical care, and careful medication review. DNA testing is optional in many cases and is most valuable when it changes a real decision.
Authoritative Outbound Sources
The following official, primary, and peer-oriented resources support the clinical framing used in this article.
- FDA – Table of Pharmacogenetic Associations
- MedlinePlus Genetics – Genetic Testing
- MedlinePlus Genetics – Types of Genetic Tests
- MedlinePlus Genetics – Interpreting Results
- MedlinePlus Genetics – Secondary Findings
- MedlinePlus Genetics – Cost and Results Timing
- MedlinePlus Genetics – Insurance Coverage
- MedlinePlus Genetics – Risks and Limitations
- NCBI Bookshelf – Clopidogrel Therapy and CYP2C19 Genotype
- Genome.gov – Genetic Discrimination and GINA
- NHGRI – DNA Sequencing Costs Data
- ACMG – Recommendations for Reporting of Secondary Findings in Clinical Exome and Genome Sequencing
- PharmGKB
- CPIC – Clinical Pharmacogenetics Implementation Consortium
Medical note: These links are provided for education and further reading. Individual genetic testing, medication, and treatment decisions should be reviewed with a qualified healthcare professional.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.