How to Prevent Sarcopenia in Older Adults
Older adults can lower sarcopenia risk by combining progressive strength training two or three days a week, balance and aerobic activity, protein-rich meals across the day, and regular monitoring of grip, chair-rise ability, walking, appetite, body weight, and falls. New or worsening weakness, unintentional weight loss, repeated falls, or swallowing problems should be reviewed by a healthcare professional.
Executive Summary
Sarcopenia is the age-related decline in muscle strength, muscle quantity, and physical performance. Current consensus guidance places low muscle strength first in case-finding because strength loss predicts disability, falls, and loss of independence more directly than muscle size alone. For a practical U.S. audience, the best prevention plan is not complicated: do muscle-strengthening work at least twice weekly, add balance training every week, walk or do other aerobic activity most days, and eat enough protein consistently rather than letting breakfast and lunch stay protein-poor.
A workable nutrition target is to move beyond the basic adult RDA of 0.8 g/kg/day and toward a more muscle-protective intake pattern if tolerated and medically appropriate. Reviews focused on older adults report that protein-and-aging experts often recommend 1.2–2.0 g/kg/day or higher for many older adults, while practical meal-based planning often starts with roughly 25–40 g of quality protein at breakfast, lunch, and dinner. For bone support alongside muscle work, NIH’s Office of Dietary Supplements lists calcium needs up to 1,200 mg/day and vitamin D needs of 800 IU/day for adults older than 70, although vitamin D alone has shown inconsistent benefits for muscle strength and functional performance.
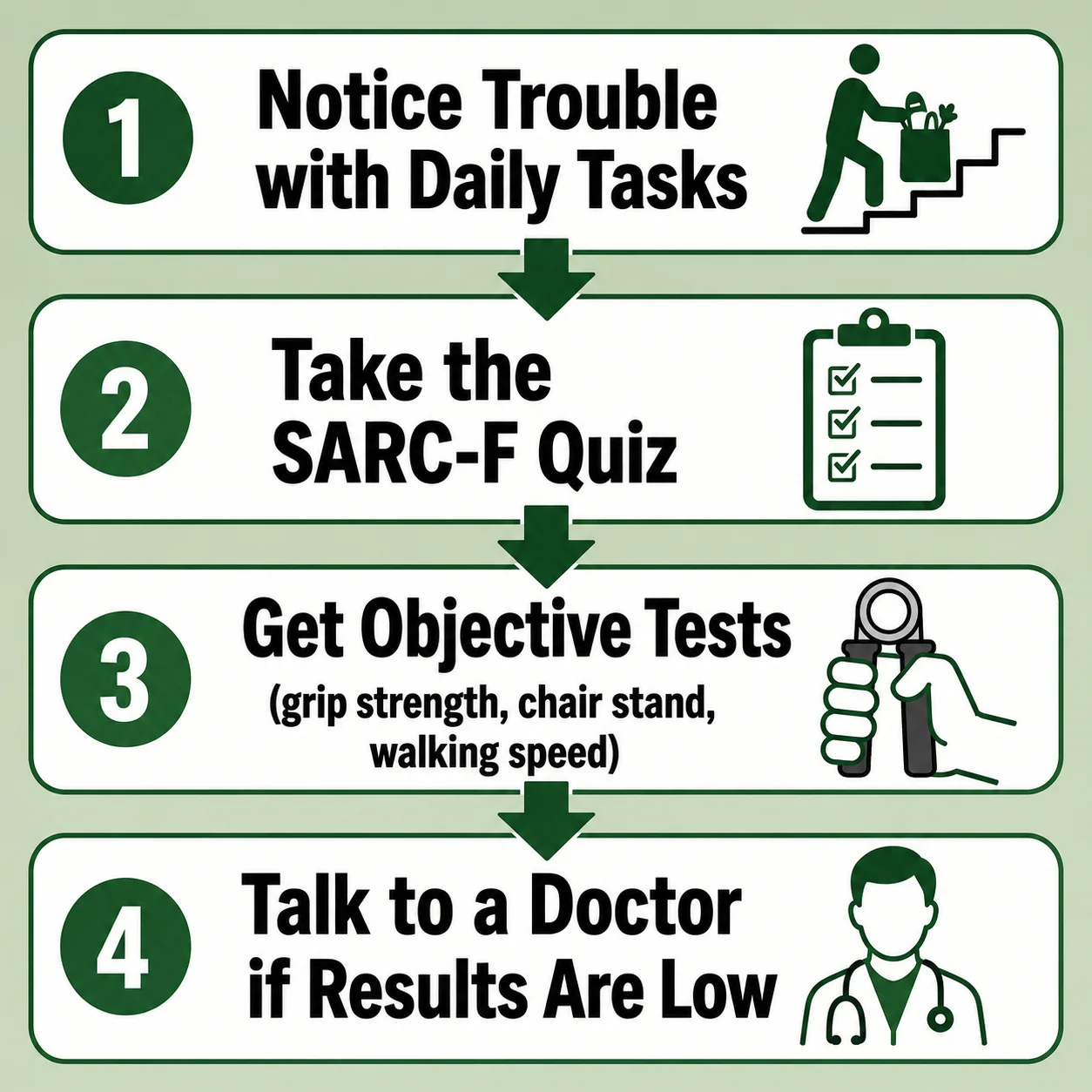
Home monitoring matters. If an older adult reports trouble carrying groceries, walking, rising from a chair, climbing stairs, or frequent falls, consensus guidance recommends a screening pathway that starts with the SARC-F questionnaire and then checks objective measures such as grip strength, chair-stand time, gait speed, the Short Physical Performance Battery, or the Timed Up and Go test. Widely used cutoffs include grip strength <27 kg for men and <16 kg for women, chair stand >15 seconds for five rises, gait speed ≤0.8 m/s, SPPB ≤8, and a CDC fall-risk flag of TUG ≥12 seconds.
How to Prevent Sarcopenia in Older Adults: What to Do Now
The most effective first move is to shift from a “light activity is enough” mindset to a muscle-preservation routine. CDC guidance for adults age 65 and older calls for aerobic activity every week, muscle-strengthening work on at least 2 days, and regular balance activities. In practice, that means a week should include walking or other aerobic movement, two or three strength sessions, and short balance drills such as tandem standing, heel-to-toe walking, or repeated sit-to-stands.
The second move is to stop saving almost all protein for dinner. Older adults often eat little protein until evening, yet age-related anabolic resistance appears to improve when total protein is higher and meals are more intentional. The evidence is not perfect on whether perfectly even distribution beats every other pattern, but reviews consistently support a higher total daily protein intake in older adults and show that a meal containing roughly 35 g of high-quality protein or about 0.40 g/kg/meal can be a strong practical target. For food ideas that make this easier, see our guide on what to eat to gain muscle after 60.
The third move is to watch function, not just body weight. A person can maintain or even gain weight while still losing muscle and function. That is why sarcopenia screening depends on what people can do: grip, chair rises, walking speed, and balance. EWGSOP2 explicitly prioritizes low muscle strength as the key characteristic of sarcopenia and uses low muscle quantity or quality to confirm the diagnosis.
The fourth move is to treat falls and near-falls as muscle and mobility warnings. CDC’s STEADI materials recommend functional assessments such as the 30-second chair stand, 4-stage balance test, and Timed Up and Go, and they also emphasize medication review because some drugs increase fall risk. If an older adult has become slower, shakier, or newly dependent on armrests to stand, that deserves action now rather than later.

How Sarcopenia Develops and How to Screen for It
Why It Matters
Consensus guidance describes sarcopenia as a muscle disease rooted in adverse muscle changes across the life course, and notes that the condition is associated with falls, fractures, lower quality of life, mobility disorders, loss of independence, and death. The same paper notes that after midlife, declines in muscle mass and strength accelerate, with reports of 1–2% annual leg muscle mass loss and roughly 1.5–5% annual strength loss beyond age 50.
For prevention writing aimed at U.S. older adults, the most helpful explanation is simple: sarcopenia is rarely caused by age alone. It is usually pushed along by a combination of inactivity, too little protein or energy, illness, hospital stays, medication burden, pain, arthritis, obesity with low muscle quality, and fear of falling that reduces movement. CDC materials for older adults emphasize that regular activity helps people keep doing day-to-day tasks without becoming dependent on others.
Validated Screening Tools and Cutoffs
The table below is the most useful clinical-to-home bridge for an article like this. It lets caregivers understand which tests are screening tools, which are fall-risk tools, and which numbers should prompt a clinician or physical therapist review.
| Tool | What It Measures | Practical Interpretation |
|---|---|---|
| SARC-F | Self-reported difficulty with strength, walking, rising from a chair, climbing stairs, and falls | Use as the first screen when symptoms are suspected; positive or concerning responses should lead to objective testing. |
| Grip strength | Upper-extremity strength, correlates with low muscle strength | Low strength cutoff: men <27 kg, women <16 kg. |
| Five-times chair stand | Leg strength and functional transfer ability | >15 seconds for five rises suggests low strength. |
| Gait speed | Physical performance and mobility reserve | ≤0.8 m/s supports poor physical performance in sarcopenia screening. |
| SPPB | Composite of gait speed, balance, and chair stand | ≤8 points indicates poor physical performance. |
| Timed Up and Go | Mobility and fall risk | CDC flags ≥12 seconds as fall risk; consensus sarcopenia frameworks often use a higher threshold, such as ≥20 seconds, for poor performance. |
| 4-stage balance test | Static balance | Inability to hold tandem stand 10 seconds increases fall risk. |
| 30-second chair stand | Leg strength and endurance | CDC provides age-based below-average ranges and advises that a below-average score signals fall risk. |
Grip-Strength Norms and Thresholds
A precise, public, government-run U.S. age-by-sex grip chart is not as easy to standardize across home devices as people expect, so the most publishable and defensible approach is to use screening thresholds plus trend monitoring. EWGSOP2 points readers to life-course normative data and displays cut-points of ≤27 kg for men and ≤16 kg for women as the practical low-strength threshold. For consumers, trend matters too: the same dynamometer, same arm position, same time of day, and watching for a meaningful decline from personal baseline.
| Grip-Strength Interpretation | Men | Women | How to Use It |
|---|---|---|---|
| Likely low muscle strength | <27 kg | <16 kg | Seek clinician/PT review and pair the result with chair-stand, gait, balance, and fall history. |
| Borderline but functional | At or above cutoff | At or above cutoff | Continue monthly tracking, especially after illness, bed rest, or unintentional weight loss. |
| Home trend warning | >5–10% drop from your typical best | >5–10% drop from your typical best | A practical self-monitoring rule; trend often matters more than one isolated reading. |
Protein Timing, Daily Targets, and Food Choices
Practical Protein Targets
The minimal adult RDA remains 0.8 g/kg/day, but reviews focused on older adults note that this level reflects the lower end of basic adequacy and may fall short of what is ideal for preserving muscle and function in aging. The same literature reports expert recommendations of 1.2–2.0 g/kg/day or higher for many older adults, especially when illness, low appetite, or recovery is part of the picture. A practical, conservative article recommendation is to help most older adults move upward from 0.8 g/kg/day toward about 1.0–1.2 g/kg/day, then individualize higher targets with a clinician or dietitian if they are frail, under-eating, or recovering from illness.
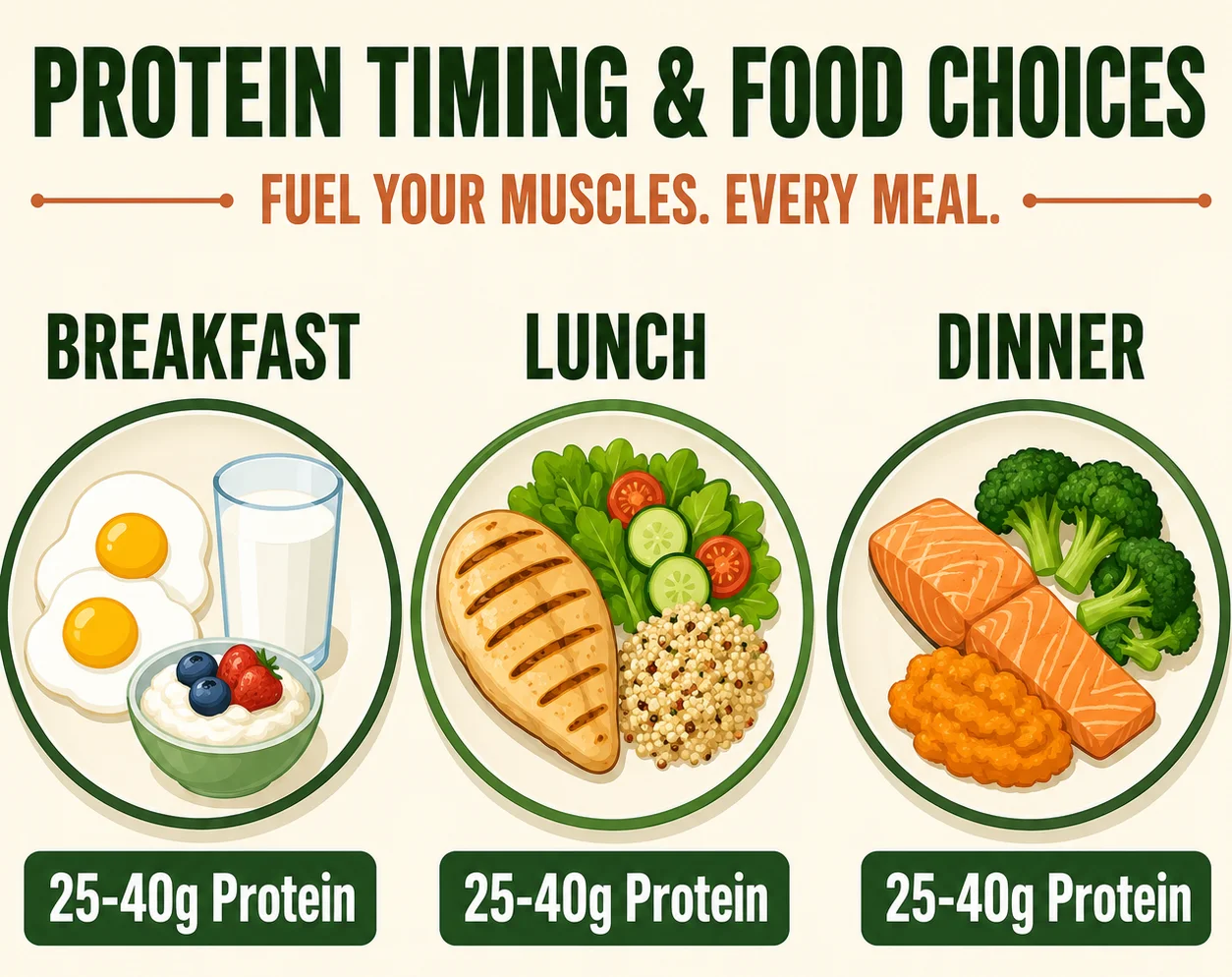
For meal timing, the most useful message is this: prioritize total daily protein first, then anchor each meal with protein. A helpful meal pattern is 25–40 g protein at breakfast, lunch, and dinner, plus a protein-rich snack if appetite is low or a strength session was completed. The older-adult protein review notes that about 35 g of high-quality protein per meal is a practical stimulus for muscle protein synthesis, while also showing that total intake across the day remains crucial.
Protein Timing That Older Adults Can Actually Follow
For publishing purposes, the cleanest recommendation is not an athlete-style nutrient-timing plan. It is this routine:
Morning: include a real protein source at breakfast. Midday: avoid a low-protein lunch made only of soup, crackers, or fruit. Evening: keep dinner protein-forward, but do not rely on dinner alone. After strength training: use the workout as a reminder to eat a protein-containing meal or snack within the next couple of hours.
That pattern is easier than telling a 76-year-old caregiver to calculate leucine grams, and it aligns with the broader evidence that older adults need more deliberate protein placement across the day than younger adults.
Protein Food List With Portions
Approximate protein values below reflect common USDA FoodData Central entries and typical U.S. package labels. For a live article, note that exact values vary by brand and preparation and link readers to FoodData Central for verification.
| Food | Typical Portion | Approx. Protein |
|---|---|---|
| Greek yogurt, plain | 1 cup | 20 g |
| Cottage cheese | 1/2 cup | 14 g |
| Milk | 1 cup | 8 g |
| Eggs | 2 large | 12 g |
| Chicken breast, cooked | 3 oz | 25–27 g |
| Salmon, cooked | 3 oz | 21–23 g |
| Lean ground beef, cooked | 3 oz | 22–24 g |
| Tofu, firm | 1/2 cup | 10–12 g |
| Edamame | 1 cup | 17–18 g |
| Lentils, cooked | 1 cup | 17–18 g |
| Black beans, cooked | 1 cup | 14–15 g |
| Peanut butter | 2 tbsp | 7 g |
| String cheese | 1 stick | 6–8 g |
| Whey or milk-based protein powder | 1 scoop | 20–25 g |
A Detailed 3-Day Meal Plan Table
This table is detailed enough to stand alone in an article and simple enough for caregivers to adapt. Protein totals are approximate and should be adjusted for body size, appetite, and medical conditions.
| Day | Breakfast | Lunch | Dinner | Snack | Approx. Daily Protein |
|---|---|---|---|---|---|
| Day one | 1 cup Greek yogurt, berries, oats, 1 tbsp chia | Turkey sandwich on whole grain bread, side salad, milk | Baked salmon, roasted potatoes, green beans | Cottage cheese with peaches | 95–105 g |
| Day two | 2 eggs, whole-grain toast, 1 cup milk | Lentil soup, tuna salad cup, fruit | Chicken breast, brown rice, broccoli | String cheese and apple | 90–100 g |
| Day three | Protein oatmeal made with milk plus peanut butter | Bean-and-cheese burrito with salsa and avocado | Lean beef stir-fry with vegetables and rice | Greek yogurt | 90–100 g |
A Practical 7-Day Meal Plan for the Full Article
A 7-day rotation helps older adults avoid the “I don’t know what to eat” problem that often leads to under-eating. This is intentionally simple and U.S.-friendly rather than gourmet.
| Day | Breakfast | Lunch | Dinner | Snack | Approx. Protein |
|---|---|---|---|---|---|
| Monday | Greek yogurt bowl with berries and oats | Turkey sandwich + milk | Salmon, potatoes, green beans | Cottage cheese | 95 g |
| Tuesday | Eggs + toast + fruit | Lentil soup + tuna salad | Chicken, rice, broccoli | Cheese stick | 92 g |
| Wednesday | Oatmeal with milk + peanut butter | Bean burrito + yogurt | Beef stir-fry | Greek yogurt | 93 g |
| Thursday | Cottage cheese + fruit + nuts | Chicken salad wrap | Tofu stir-fry with edamame | Milk + crackers | 90 g |
| Friday | Greek yogurt parfait | Tuna melt + tomato soup | Turkey meatballs + pasta + salad | Peanut butter toast | 94 g |
| Saturday | Egg scramble with cheese | Chickpea bowl + milk | Pork loin or fish + sweet potato | Cottage cheese | 92 g |
| Sunday | Protein smoothie + toast | Leftover salmon salad | Roast chicken + vegetables | Yogurt | 90 g |
A useful side note for the article is that bone support still matters. NIH’s Office of Dietary Supplements lists calcium needs up to 1,200 mg/day and vitamin D 800 IU/day for adults over 70, but those nutrients support the plan; they do not replace resistance training and adequate protein. For more on this, see our guide to preventing osteoporosis after menopause.
The Best Exercises and a 12-Week Progression
What the Exercise Program Should Emphasize
CDC guidance for adults 65 and older recommends 150 minutes of moderate aerobic activity, or 75 minutes of vigorous activity, plus strengthening activities on at least 2 days and balance work each week. For sarcopenia prevention, the article should tell readers to put the highest priority on progressive resistance work for major muscle groups, especially legs, hips, back, chest, shoulders, and arms, because those muscle groups matter most for rising, climbing, carrying, and preventing falls. Building and maintaining this muscle also supports a healthy metabolic rate after 60.
The simplest home program uses movements that map directly to daily function: sit-to-stand, squat-to-chair, step-up, push, pull, carry, calf raise, and balance drills. CDC’s older-adult activity examples specifically mention sit-to-stand and heel-to-toe walking as balance-related activities, and CDC STEADI provides chair stand, balance, and TUG assessments that can double as training benchmarks.
Sample Home Exercise Program
A publishable home program for beginners should be framed as 2 or 3 nonconsecutive strength days per week, with a separate short balance routine at least 3 days per week, and walking or cycling most days as able. Start with 1–2 sets of 8–12 repetitions for most exercises, stopping with good form still intact. When the top number of repetitions feels manageable for two sessions in a row, increase the load, use a stronger resistance band, slow the lowering phase, or move to a harder variation such as wall push-up to counter push-up, or chair squat to unassisted squat. That is progressive overload translated into plain language. For budget-friendly ways to support this routine with food, see our guide on rebuilding muscle after 60 with cheap everyday foods.
Exercise Progression Table
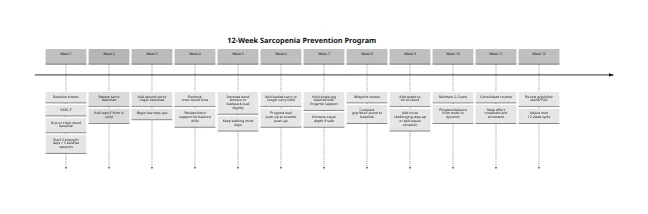
| Phase | Weeks | Goal | Strength Work | Balance Work | Progression Rule |
|---|---|---|---|---|---|
| Foundation | 1–2 | Learn form and build routine | Chair sit-to-stand, wall push-up, seated band row, calf raise, supported hip hinge | Feet together stand, heel-to-toe walk at counter | Add 1–2 reps each session if form stays solid |
| Build | 3–4 | Increase total work | Sit-to-stand 2 sets, counter push-up, standing band row, step-up to low step, calf raise 2 sets | Tandem stand, marching in place, side steps | Move from 1 to 2 sets and reduce hand support |
| Strengthen | 5–8 | Add resistance and control | Goblet-style chair squat or backpack squat, band chest press, one-arm row, split squat to chair, hip hinge with weight | Single-leg stand with fingertip support, turn-and-step drills | Increase band tension or backpack load by a small amount |
| Power and function | 9–12 | Improve confidence and daily function | Faster sit-to-stand, step-up, loaded carry, row, press, calf raise, hip hinge | Dynamic balance: tandem walk, heel raise holds, obstacle stepping | Keep 2–3 sets and progress difficulty only if no increase in pain or instability |
Safety Modifications
For adults with arthritis, shorter ranges of motion and slower tempo are often better at the start. For adults with osteoporosis or vertebral fracture risk, avoid aggressive twisting and loaded forward bending without clinician guidance. For people with neuropathy or poor balance, keep a countertop, rail, or sturdy chair nearby. For anyone returning after hospitalization, begin with chair stands, supported walking, and one resistance exercise per major pattern rather than trying a full circuit on day one. CDC STEADI emphasizes staying beside the patient for safety during chair-stand, balance, and TUG testing, which is also good advice for early home training.
12-Week Sarcopenia Prevention Timeline
Monitoring Progress and Knowing When to Seek Medical Review
A Simple Monitoring Checklist
A high-performing article for older adults should give readers a checklist they can actually print or copy into a notebook. The one below aligns with CDC functional testing and the consensus approach to monitoring low strength and performance.
| What to Track | How Often | Goal |
|---|---|---|
| Strength sessions completed | Weekly | 2–3 sessions |
| Balance sessions completed | Weekly | 3+ short sessions |
| Walking or other aerobic minutes | Weekly | Progress toward 150 min moderate activity if able |
| Daily protein intake | Daily | Consistent protein at all 3 meals |
| Body weight | Weekly | Avoid unexplained downward trend |
| Grip strength | Monthly | Stable or improving from baseline |
| Five chair rises or 30-second chair stand | Monthly | Faster or more repetitions over time |
| Falls or near-falls | Ongoing | Zero if possible; any new fall should trigger review |
| Medication changes | Ongoing | Note if new sedatives or dizziness begin |
| Appetite and chewing/swallowing ability | Ongoing | Address early before intake drops |
When a Clinician or Therapist Should Get Involved
Medical review is warranted if an older adult has new or progressive weakness, recurrent falls, TUG ≥12 seconds, trouble holding tandem stand for 10 seconds, or a clearly abnormal grip or chair-stand result. It is also wise to seek review if the person is unintentionally eating less, losing weight, becoming dependent on their arms to stand, or starting medications linked to dizziness or fall risk. CDC STEADI explicitly includes functional assessments and medication review as part of fall-risk management.
Urgent medical review is more appropriate when weakness is accompanied by sudden one-sided symptoms, chest pain, severe shortness of breath, dark urine after exertion, severe dehydration, new confusion, or trouble swallowing enough to stay hydrated or nourished. Those red flags suggest something beyond ordinary deconditioning and should not be labeled “just aging.”
If screening remains concerning, the next clinical step can include confirmation of low muscle quantity or quality with DXA or BIA in usual care, and sometimes MRI or CT in specialty settings. That is the consensus pathway after probable sarcopenia has been identified.

FAQs
Begin with two weekly strength sessions, regular balance practice, and three protein-anchored meals per day. Those steps address the main modifiable drivers of age-related muscle loss.
The adult RDA is 0.8 g/kg/day, but many experts in protein and aging recommend higher targets for older adults, often around 1.2–2.0 g/kg/day, depending on health status and clinician guidance.
Yes, but total daily protein matters first. A practical plan is to include protein at breakfast, lunch, and dinner rather than saving almost all of it for dinner.
A practical target is about 25–40 g of quality protein at a meal, with around 35 g often used as a useful benchmark in older-adult nutrition reviews.
The best exercise category is progressive resistance training, especially moves that train standing up, climbing, carrying, pushing, and pulling. Balance work should be added every week.
Yes. CDC guidance for adults 65 and older specifically includes balance activity every week because walking alone may not challenge balance enough to reduce fall risk.
SARC-F is a five-item self-report screen that asks about strength, walking ability, rising from a chair, stair climbing, and falls. It is commonly recommended for sarcopenia case-finding.
Commonly used cutoffs are below 27 kg for men and below 16 kg for women. A result below those thresholds should prompt clinical follow-up rather than panic.
Use a five-times chair-stand test or the CDC 30-second chair-stand format. Trouble standing without the arms, slow performance, or downward trends over time are meaningful warning signs.
CDC recommends at least 150 minutes of moderate aerobic activity or 75 minutes of vigorous activity weekly, plus muscle-strengthening work on at least 2 days and balance activities.
No. Calcium and vitamin D support bone health, but they do not substitute for resistance training and adequate protein. Evidence for vitamin D alone improving muscle performance in older adults is inconsistent.
Start with the easiest protein wins: Greek yogurt, milk, eggs, cottage cheese, soups with beans or lentils, and softer fish or poultry. Small protein-rich meals are better than waiting for a large dinner.
See a PT if standing from a chair is difficult, a fall has happened, balance is worsening, or walking is becoming slower and less confident. CDC’s STEADI framework supports using functional tests to guide intervention.
Yes. Medication burden and certain fall-linked drugs can worsen dizziness, balance, and functional decline, so medication review should be part of the plan.
It can improve or at least be slowed. Consensus guidance notes that early and effective intervention, especially nutrition and exercise, can prevent, delay, and sometimes reverse clinically important decline.
Authoritative Outbound Sources Used
The following government, clinical, nutrition, and peer-reviewed resources support the article’s recommendations on physical activity, sarcopenia screening, protein intake, fall prevention, and healthy aging.
- CDC – Physical Activity Guidelines for Older Adults
- EWGSOP2 – Sarcopenia: Revised European Consensus on Definition and Diagnosis
- CDC STEADI – Clinical Resources for Fall Prevention
- National Institute on Aging – Exercise and Physical Activity
- Nutrients – Protein Consumption and the Elderly: What Is the Optimal Level of Intake?
- USDA FoodData Central
- USDA MyPlate – Older Adults
- NIH Office of Dietary Supplements – Calcium
- NIH Office of Dietary Supplements – Vitamin D
- USPSTF – Falls Prevention in Community-Dwelling Older Adults
Medical note: These links are provided for education and further reading. Individual protein, exercise, fall-prevention, and treatment decisions should be reviewed with a qualified healthcare professional.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.