The thyroid gland plays a crucial role in regulating the body’s metabolism, energy levels, and overall hormonal balance. When it malfunctions — producing either too much or too little hormone — the effects ripple through virtually every system in the body. Recognizing the symptoms of thyroid issues early is essential, because thyroid disorders are among the most common endocrine conditions in the United States, affecting an estimated 20 million Americans, yet up to 60% of those with thyroid disease are unaware of their condition.
The thyroid is a butterfly-shaped gland located at the base of the neck, just below the Adam’s apple. It produces two primary hormones — thyroxine (T4) and triiodothyronine (T3) — which regulate the rate at which every cell in the body uses energy. Think of the thyroid as the body’s metabolic thermostat: when it runs too hot (hyperthyroidism) or too cold (hypothyroidism), the downstream effects are far-reaching and can mimic dozens of other conditions, making thyroid disorders notoriously difficult to diagnose without laboratory testing.
This article focuses primarily on hyperthyroidism — the overactive thyroid state — which is most commonly caused by Graves’ disease (an autoimmune condition), toxic multinodular goiter, or thyroiditis. Women are five to eight times more likely than men to develop hyperthyroidism, and the condition becomes more prevalent after age 60, making it particularly relevant for older adults who may dismiss its symptoms as normal aging.
Because hyperthyroidism affects so many body systems simultaneously, its symptoms are wide-ranging and vary significantly between individuals. The sections below cover each major symptom category in depth, so you can build a complete picture of what an overactive thyroid looks and feels like — and know when to seek testing.
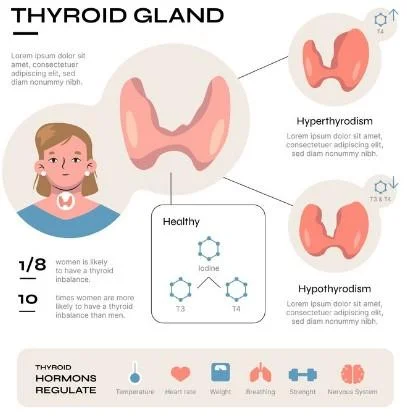
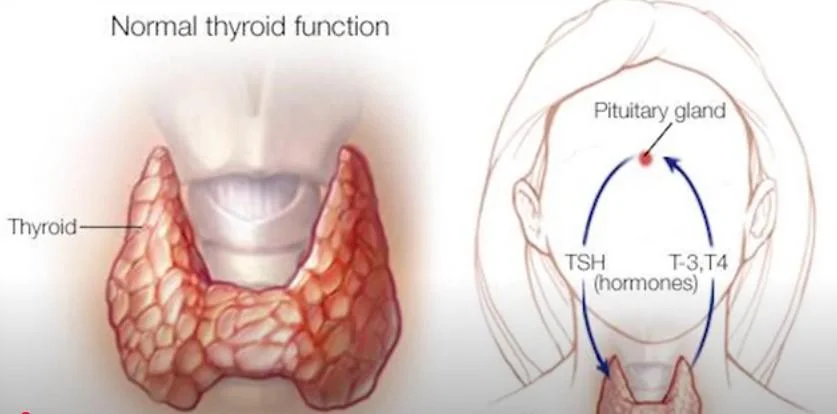
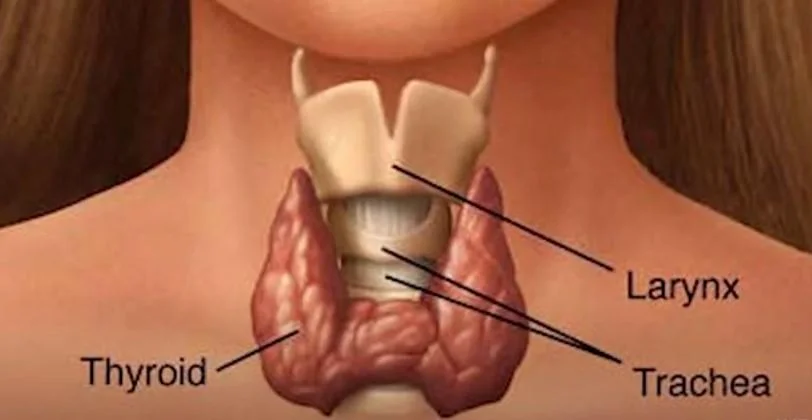
Table of Contents
- Recognizing Hyperthyroidism Symptoms
- Eye-Related Symptoms
- Hair and Skin Issues
- Weight Changes and Appetite
- Fatigue and Energy Levels
- Cardiovascular Symptoms
- Digestive Symptoms
- Neurological and Cognitive Effects
- Temperature Regulation
- Muscle and Joint Symptoms
- Other Notable Symptoms
- Clinical Signs and Diagnosis
- Managing Hyperthyroidism
- When to Seek Help
Recognizing Hyperthyroidism Symptoms
Hyperthyroidism occurs when the thyroid gland produces excessive hormones, leading to an overactive metabolism. Common symptoms span multiple body systems and can develop gradually or appear suddenly depending on the underlying cause.
The hallmark of hyperthyroidism is a body running in a state of metabolic overdrive. Excess thyroid hormone accelerates nearly every physiological process: the heart beats faster, food moves through the digestive tract more quickly, muscles break down at an increased rate, and the nervous system becomes hyperactivated. This explains why hyperthyroidism symptoms can seem scattered across so many different organ systems — they all share the same root cause: too much thyroid hormone signaling.
Graves’ disease — the most common cause of hyperthyroidism in the United States — is an autoimmune condition in which the immune system produces antibodies that mimic thyroid-stimulating hormone (TSH), continuously signaling the gland to produce more T3 and T4. It accounts for 70–80% of all hyperthyroidism cases and has a strong genetic component: if a close family member has Graves’ disease or another autoimmune thyroid condition, your risk is meaningfully elevated.
A key diagnostic concept: because many hyperthyroidism symptoms overlap with anxiety, depression, perimenopause, cardiovascular disease, and other common conditions, thyroid disorders are frequently missed or misdiagnosed for months to years. If you recognize a cluster of the symptoms described below — particularly in combination — asking your doctor for a simple TSH blood test is a reasonable and important step. TSH testing is inexpensive, widely available, and the most sensitive indicator of thyroid dysfunction.
Eye-Related Symptoms
Hyperthyroidism eyes are a common early indicator. Many individuals experience bulging eyes (exophthalmos), especially in Graves’ disease. Graves disease eye swelling and early Graves disease eyes may also cause discomfort, dry eyes, or irritation. Eyelid lag hyperthyroidism and dry eyes and hyperthyroidism are other notable symptoms.
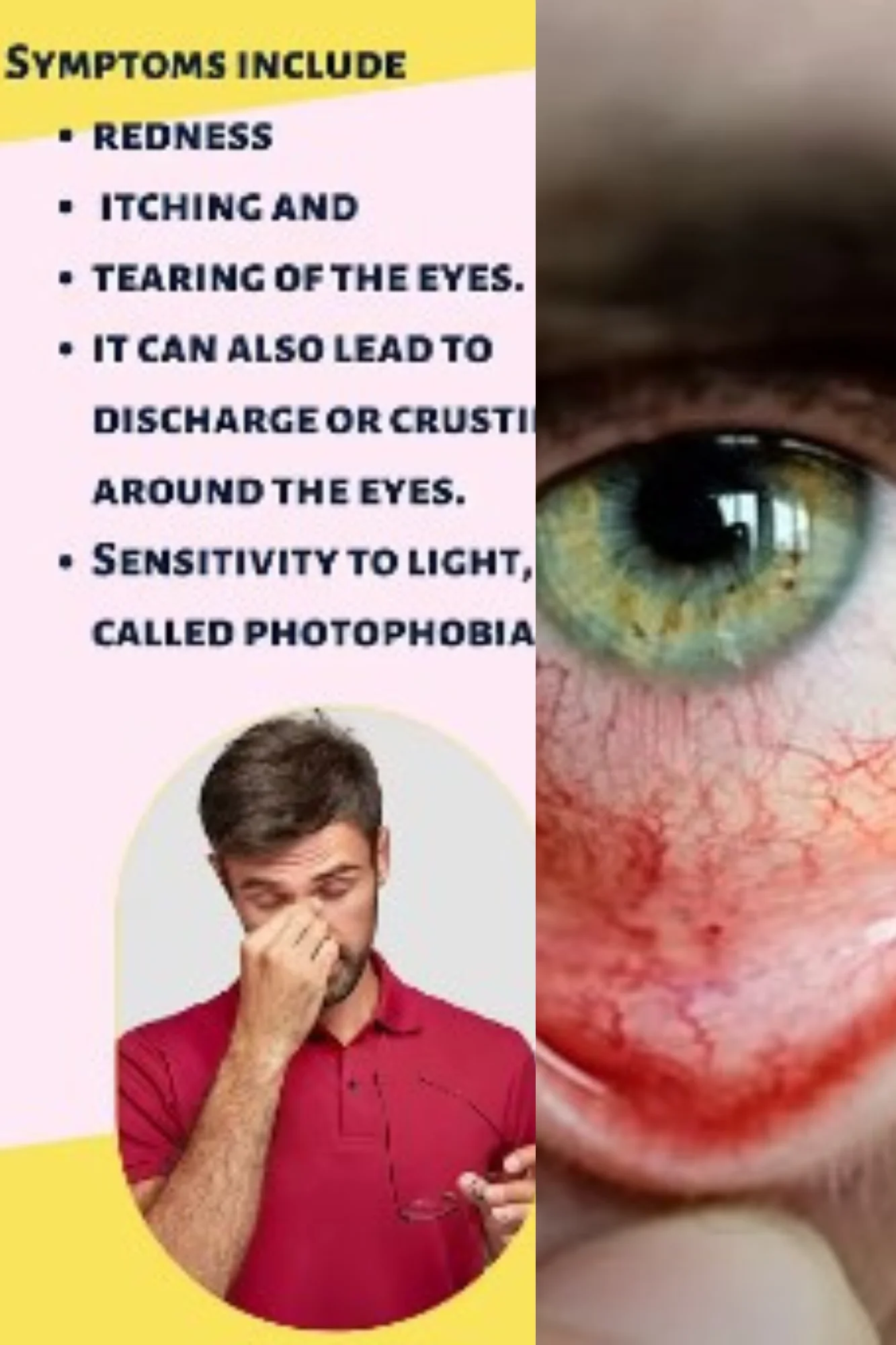
Thyroid eye disease (TED), also called Graves’ ophthalmopathy, occurs in approximately 25–50% of people with Graves’ disease and can sometimes precede the thyroid diagnosis by months. It results from immune cells infiltrating the tissues behind the eye — the orbital fat and eye muscles — causing them to swell and push the eyeball forward. The medical term for this protrusion is proptosis or exophthalmos, and it is one of the most recognizable external signs of Graves’ disease.
Beyond appearance, TED can cause significant functional impairment: double vision (diplopia) from swollen eye muscles, exposure keratopathy (corneal damage from eyes that don’t close fully during sleep), and in severe cases, optic nerve compression that can threaten vision. A 2020 clinical guideline from the European Group on Graves’ Orbitopathy recommends all patients with newly diagnosed Graves’ disease receive formal ophthalmological assessment, regardless of whether they notice eye symptoms — because early, subtle changes may not be obvious to the patient.
Eyelid lag — where the upper eyelid lags behind the eye when looking downward — is a distinctive sign that eye specialists specifically look for. It results from excess sympathetic nervous system stimulation causing the eyelid retractor muscles to remain overactivated. If you notice that your eyes appear more prominent than usual, feel gritty or dry, or tear excessively, these warrant an evaluation by both an endocrinologist and an ophthalmologist familiar with thyroid eye disease.
Hair and Skin Issues
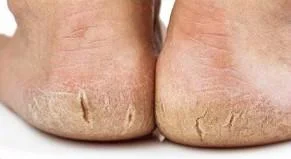
Hyperthyroidism hair loss and hair thinning hyperthyroidism are common, often leading to noticeable shedding or bald patches. Dry skin hyperthyroidism and hyperthroid itchy skin can occur as the condition progresses. Some patients report skin rash hyperthyroidism or hives associated with the condition.

Hair loss in hyperthyroidism — termed telogen effluvium — occurs because excess thyroid hormone disrupts the normal hair growth cycle, pushing a larger-than-normal proportion of hair follicles into the resting (telogen) phase simultaneously. The result is diffuse hair shedding across the entire scalp rather than the patchy loss seen in alopecia areata. Crucially, this shedding often peaks 2–3 months after the triggering event — meaning people sometimes notice significant hair loss just as their thyroid is being treated, which can be alarming but is actually a delayed consequence of the earlier hormonal disruption.
Skin changes in Graves’ disease include a distinctive condition called pretibial myxedema — a thickening and reddening of the skin on the shins, sometimes described as having an orange-peel texture. Despite “myxedema” being a term more associated with hypothyroidism, pretibial myxedema is paradoxically a feature of Graves’ disease and occurs in approximately 5% of cases. It is an immune-mediated process distinct from the direct hormonal effects of excess thyroid hormone.
For women experiencing hair thinning who attribute it solely to aging or menopause, thyroid function testing is a straightforward and important step. The American Academy of Dermatology notes that thyroid disorders are among the top reversible causes of hair loss in adult women, and that hair regrowth typically occurs — often within 6–12 months — once thyroid hormone levels are restored to normal through treatment.
Weight Changes and Appetite
Despite increased appetite, many individuals experience hyperthyroidism and weight loss due to a heightened metabolic rate. Conversely, hyperthyroidism cause weight gain may occur in rare cases. Symptoms like hyperthyroidism appetite loss can also impact nutritional health.

Unexplained weight loss — particularly when accompanied by increased appetite rather than decreased food intake — is one of the most clinically significant warning signs of hyperthyroidism. Excess thyroid hormone increases the basal metabolic rate (the number of calories the body burns at rest), meaning the body effectively consumes its own fat and muscle tissue even when caloric intake is normal or increased. Weight losses of 10–20 pounds over several months without dietary changes are not uncommon in untreated hyperthyroidism.
The paradoxical weight gain seen in a minority of hyperthyroid patients typically occurs when the increased appetite that accompanies the condition outpaces the elevated metabolic burn — a pattern more common in younger patients or in cases where anxiety and stress-eating behaviors intensify alongside the hormonal changes. This can lead to a delayed or missed diagnosis when clinicians expect weight loss and observe weight gain instead.
Nutritional management during hyperthyroid treatment is an underappreciated aspect of care. Because the hypermetabolic state depletes calcium, vitamin D, and muscle mass, patients being treated for hyperthyroidism should discuss bone health monitoring and nutritional support with their endocrinologist. A diet adequate in protein (to support muscle preservation), calcium (1,000–1,200 mg/day for adults over 50), and vitamin D is particularly important during and after treatment.
Fatigue and Energy Levels
Extreme fatigue hyperthyroidism and fatigue with hyperthyroidism are hallmark signs. Many individuals feel constant tiredness despite rest, often linked to hyperthyroidism and exhaustion.
It may seem counterintuitive that an overactive thyroid — a condition of metabolic excess — causes profound fatigue, but this is one of its most consistent and debilitating features. The fatigue of hyperthyroidism results from several converging factors: disrupted sleep (insomnia and restlessness are common), excessive cardiovascular strain that leaves the heart and muscles chronically overworked, and the depletion of muscle mass and energy stores caused by the hypermetabolic state. The body is running at full throttle all the time, and eventually the fuel runs out.
This fatigue is qualitatively different from ordinary tiredness. Patients frequently describe it as a bone-deep exhaustion that is not relieved by sleep, accompanied by muscle weakness — particularly in the upper arms and thighs — that can make climbing stairs, lifting groceries, or rising from a chair surprisingly difficult. Proximal muscle weakness (affecting the muscles closest to the body’s core) is a recognized complication of hyperthyroidism called thyrotoxic myopathy, and it can be severe enough to limit daily functioning.
If you are experiencing persistent fatigue that doesn’t improve with adequate sleep, particularly if accompanied by any of the other symptoms in this article, thyroid function testing should be on your diagnostic checklist. The TSH test required is a simple blood draw that can be ordered by any primary care physician.
Cardiovascular Symptoms
Heart palpitations and hyperthyroidism and increased heart rate in hyperthyroidism are common. Severe cases may lead to heart failure and hyperthyroidism, requiring immediate medical attention.
The cardiovascular system is one of the most immediately and seriously affected by excess thyroid hormone. Thyroid hormones directly increase the number and sensitivity of beta-adrenergic receptors on heart muscle cells, making the heart more responsive to adrenaline. The result is a resting heart rate that may be elevated to 90–130 beats per minute (normal is 60–100), along with forceful palpitations — the sensation that the heart is pounding, racing, or skipping beats.
Most significantly, hyperthyroidism is a well-established risk factor for atrial fibrillation (AFib) — an irregular, often rapid heart rhythm that can lead to stroke, heart failure, and other serious complications. AFib occurs in approximately 10–15% of patients with overt hyperthyroidism and up to 25% of those with subclinical (mild) hyperthyroidism over age 60. This is a critical reason why thyroid function should be checked in any older adult newly diagnosed with AFib, and why untreated hyperthyroidism in older patients is genuinely dangerous.
If you experience new or worsening palpitations, a feeling that your heart is racing or fluttering, shortness of breath on exertion, or ankle swelling in the context of thyroid symptoms, seek medical evaluation promptly. These symptoms can indicate thyroid-related AFib or early heart failure — both of which are treatable but require timely intervention. Do not wait for a scheduled appointment if these symptoms are severe or sudden in onset; go to an urgent care or emergency department.
Digestive Symptoms
Diarrhea hyperthyroidism, constipation hyperthyroidism, and acid reflux hyperthyroidism are gastrointestinal signs of thyroid dysfunction. Some experience hyperthyroidism vomiting or cough and hyperthyroidism as additional symptoms.

Thyroid hormone accelerates gastrointestinal motility — the rate at which food and waste move through the digestive tract. In hyperthyroidism, this acceleration manifests most commonly as increased bowel frequency (having 3 or more loose stools per day) or frank diarrhea. Some patients experience urgency — a sudden, difficult-to-defer need to defecate — that can be socially disruptive and anxiety-provoking. These digestive changes result from both the direct effect of thyroid hormone on intestinal smooth muscle and an increase in bile production that alters stool consistency.
Acid reflux in hyperthyroidism occurs through multiple mechanisms: increased gastric acid production, relaxation of the lower esophageal sphincter (the valve between the stomach and esophagus), and potentially faster gastric emptying that paradoxically promotes reflux episodes. Patients who notice new or worsening heartburn alongside other hyperthyroid symptoms should discuss thyroid testing with their physician rather than assuming the reflux is a standalone condition.
Unexplained weight loss combined with increased bowel frequency is a symptom combination that warrants thorough evaluation — it overlaps not only with hyperthyroidism but also with other conditions (celiac disease, inflammatory bowel disease, malabsorption syndromes) that a physician will want to exclude. A comprehensive workup including thyroid function tests and other blood work is the appropriate first step.
Neurological and Cognitive Effects
Cognitive issues like brain fog hyperthyroidism and memory loss are frequently reported. Neurological symptoms such as dizziness with hyperthyroidism, vertigo, or numbness may develop. Hyperthyroid and insomnia or sleeplessness can severely disrupt sleep patterns.

The neurological and cognitive effects of hyperthyroidism are among the most distressing for patients, precisely because they are least expected from a “thyroid problem.” Excess thyroid hormone creates a state of chronic sympathetic nervous system activation — essentially, the body’s fight-or-flight response is turned up continuously. This manifests as anxiety, irritability, restlessness, difficulty concentrating, and cognitive “noise” that makes focused thinking difficult. Many patients describe it as feeling mentally wired but unable to think clearly — a combination of hyperactivation and inefficiency.
Insomnia is nearly universal in active hyperthyroidism. The combination of elevated heart rate, sweating, restlessness, and anxious rumination makes it difficult to fall or stay asleep. Chronic sleep deprivation then compounds the fatigue, cognitive impairment, and mood disturbance, creating a vicious cycle. Importantly, insomnia in hyperthyroidism typically resolves completely once thyroid hormone levels are normalized — a reassuring fact for patients who may fear they are developing a chronic sleep disorder.
Fine tremor — a subtle but rapid shaking of the outstretched hands — is one of the most specific neurological signs of hyperthyroidism and is present in the majority of cases. It results from increased beta-adrenergic receptor sensitivity in skeletal muscle. Patients often first notice it when holding a cup of coffee or trying to thread a needle. If a physician holds a sheet of paper against the patient’s outstretched hands, the tremor becomes clearly visible. This is a straightforward clinical finding that should prompt thyroid function testing if no other cause is apparent.
Temperature Regulation
Heat intolerance hyperthyroidism is a classic symptom where individuals feel excessively warm even in normal temperatures. Hyperthyroidism sweat, night sweats, and changes in body temperature often accompany this.

Heat intolerance is one of the most consistent and recognizable features of hyperthyroidism, and it stems directly from the elevated metabolic rate. Just as a car engine running at high RPM generates more heat, a body with excess thyroid hormone produces more metabolic heat than normal — heat that must be dissipated through sweating and peripheral vasodilation (widening of blood vessels near the skin). Patients feel warm when others around them feel comfortable, prefer cool rooms and cold drinks, and may remove layers of clothing in situations where others are adding them.
Excessive sweating — hyperhidrosis — in hyperthyroidism is generalized (affecting the whole body) rather than localized, and is often most noticeable at night when the body naturally attempts to thermoregulate during sleep. Drenching night sweats that require changing nightclothes or bedding are a significant symptom that always warrants medical evaluation. In women around the age of menopause, hyperthyroid night sweats are frequently (and understandably) attributed to hormonal fluctuations — which is one reason thyroid function testing should be part of any menopause-related workup.
A practical self-assessment question: Have you recently found yourself consistently warmer than the people around you — keeping the thermostat lower than before, being the only one who finds a room too warm, or avoiding warm weather or hot drinks that previously didn’t bother you? This pattern of new-onset heat intolerance, particularly in combination with any other symptoms in this article, is a clear signal to discuss thyroid testing with your doctor.
Muscle and Joint Symptoms
Muscle-related symptoms include hyperthyroidism and muscle cramps, muscle pain, and muscle twitching. Hyperthyroidism and joint aches or edema and hyperthyroidism may also be present.

Muscle weakness in hyperthyroidism — thyrotoxic myopathy — is more prevalent than many patients or even physicians realize, affecting up to 80% of people with overt hyperthyroidism to some degree. It predominantly affects the proximal muscles: the shoulder girdle, upper arms, hip flexors, and thighs. Patients notice difficulty with tasks that require sustained use of these muscle groups — lifting arms overhead, climbing stairs, rising from a low chair, or walking uphill. In severe cases, the weakness can be profound enough to be mistaken for a primary neurological or rheumatological condition.
Muscle twitching (fasciculations) and cramps in hyperthyroidism result from altered electrolyte balance — particularly calcium and potassium dysregulation — and from the direct effect of thyroid hormone on neuromuscular excitability. These symptoms can be uncomfortable and sleep-disrupting, and they typically resolve with normalization of thyroid hormone levels, though recovery of full muscle mass and strength may take several months after treatment.
Joint symptoms in Graves’ disease — including aching, stiffness, and occasional swelling — are less well understood but are likely immune-mediated, given that Graves’ is fundamentally an autoimmune condition. They tend to improve with treatment of the underlying thyroid disorder, though some patients may have co-existing autoimmune arthritis that warrants separate evaluation and management by a rheumatologist.
Other Notable Symptoms
Hyperthyroidism and palpitations or shortness of breath and hyperthyroidism can impact daily activities. Uncommon symptoms like hyperthyroidism tingling, hyperthyroidism thirst, and hyperthyroidism throat pain may also develop.
Shortness of breath in hyperthyroidism can arise from several mechanisms working simultaneously: the elevated heart rate increases cardiac oxygen demand, the respiratory muscles (which are affected by thyrotoxic myopathy) may tire more easily, and in some cases pulmonary arterial pressure increases, reducing exercise capacity. Many hyperthyroid patients find that activities that were previously effortless — a short walk, climbing a flight of stairs — now leave them winded. This is not “just aging” — it is a physiological consequence of an overworked cardiovascular system.
Increased thirst in hyperthyroidism results from the combination of excessive sweating, increased urinary output (a consequence of elevated cardiac output and renal blood flow), and possibly a mild central effect on thirst regulation. While not as prominent a symptom as in diabetes, persistent new-onset thirst should be noted and mentioned to a physician, particularly when accompanied by other thyroid symptoms.
Throat pain or a sensation of pressure in the neck may indicate thyroiditis — inflammation of the thyroid gland — which can cause transient hyperthyroidism as damaged thyroid tissue releases stored hormone into the bloodstream. Thyroiditis is sometimes triggered by a viral illness, pregnancy (postpartum thyroiditis), or certain medications. Unlike Graves’ disease, thyroiditis-related hyperthyroidism is often self-limiting, resolving over weeks to months, though it may be followed by a period of hypothyroidism before thyroid function normalizes.
Clinical Signs and Diagnosis
Diagnosing hyperthyroidism often involves evaluating clinical signs of hyperthyroidism, including physical examination and patient history. Laboratory tests measuring TSH levels are critical. High TSH in hyperthyroidism may point to primary hyperthyroidism, while imaging can confirm thyrotoxicosis signs and symptoms. Prognosis for hyperthyroidism depends on early diagnosis and appropriate treatment.
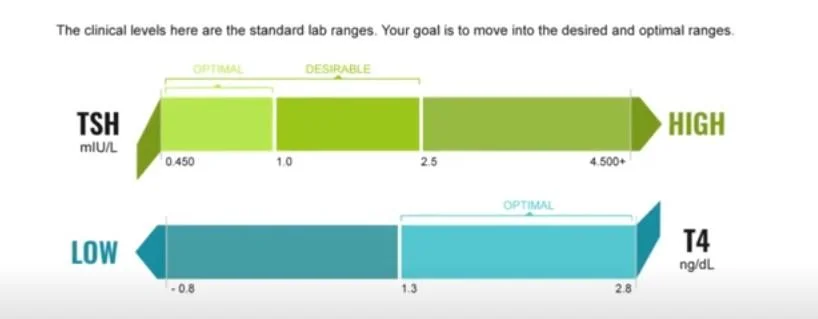
The diagnostic pathway for hyperthyroidism begins with a TSH (thyroid-stimulating hormone) blood test. In hyperthyroidism, TSH is suppressed — typically below 0.4 mIU/L, and often undetectably low — because the pituitary gland senses excess thyroid hormone in the bloodstream and reduces its own TSH output accordingly. A low TSH is then followed by measurement of free T4 and free T3 to confirm and quantify the degree of hyperthyroidism.
Once biochemical hyperthyroidism is confirmed, identifying the cause guides treatment selection. Thyroid antibody testing (TSH receptor antibodies, or TRAb) helps diagnose Graves’ disease. A radioactive iodine uptake scan differentiates between Graves’ disease (diffusely elevated uptake), toxic nodular goiter (focal uptake in nodules), and thyroiditis (suppressed uptake, since an inflamed gland cannot trap iodine normally). Thyroid ultrasound may also be used to assess gland size and nodule characteristics.
Treatment options for hyperthyroidism include antithyroid medications (methimazole or propylthiouracil), radioactive iodine ablation (which destroys overactive thyroid tissue), and surgical thyroidectomy. Each has a distinct risk-benefit profile depending on the cause of hyperthyroidism, the patient’s age, pregnancy status, and other medical conditions. Beta-blockers are frequently used in the short term to control cardiovascular symptoms (palpitations, tremor, anxiety) while definitive treatment takes effect. The choice of definitive therapy should be made collaboratively between patient and endocrinologist.
Managing Hyperthyroidism
Understanding the effects of an overactive thyroid and addressing symptoms promptly is essential. Lifestyle changes, medical interventions, and monitoring hyperthyroidism symptoms can improve quality of life significantly.
Beyond medical treatment, lifestyle modifications can meaningfully support recovery and quality of life during the hyperthyroid period. Calcium and vitamin D supplementation is particularly important: hyperthyroidism accelerates bone turnover and reduces bone density, increasing fracture risk — a concern especially relevant for postmenopausal women who already face age-related bone loss. A DEXA scan to assess bone density is often recommended for patients with prolonged hyperthyroidism or after definitive treatment.
Stress reduction and sleep hygiene are not minor lifestyle suggestions — they are genuine clinical priorities in hyperthyroidism management. Chronic stress activates the sympathetic nervous system in ways that compound the sympathetic overdrive of hyperthyroidism. Mindfulness meditation, gentle yoga, diaphragmatic breathing exercises, and consistent sleep schedules have all demonstrated measurable effects on thyroid-related symptom burden in small clinical studies.
Patients who are ultimately treated with radioactive iodine or thyroidectomy will typically develop hypothyroidism (underactive thyroid) afterward, requiring lifelong thyroid hormone replacement with levothyroxine. This is not a treatment failure — it is the expected and intended outcome for most definitive therapies. With proper dosing and regular TSH monitoring, most patients on levothyroxine live entirely normal lives with no ongoing thyroid symptoms.
When to Seek Help
If you experience persistent symptoms such as extreme fatigue, heart palpitations, or dry eyes, consult a healthcare provider promptly. Identifying the reason for hyperthyroidism early can prevent complications and promote better health outcomes.
The threshold for seeking medical evaluation should be low — not because hyperthyroidism is always dangerous, but because it is so treatable when caught appropriately and so harmful to multiple organ systems when left unaddressed. A simple TSH blood test can confirm or rule out thyroid dysfunction in a single morning blood draw, and the cost of doing nothing — prolonged cardiovascular strain, bone loss, muscle wasting, sleep deprivation, and cognitive impairment — is far higher than the cost of testing.
Seek urgent or emergency care if you experience: a heart rate above 150 beats per minute, chest pain, severe shortness of breath, confusion, fever, or profuse sweating alongside extreme agitation. These can be signs of thyroid storm — a rare but life-threatening medical emergency in which thyroid hormone levels surge precipitously, overwhelming the cardiovascular and nervous systems. Thyroid storm requires immediate hospitalization and intensive medical management.
For everyone else: make the call, request the test, and trust the information your body is giving you. Thyroid disorders are among the most manageable of chronic conditions when diagnosed and treated properly — and recognizing the symptoms is the essential first step.
This article is for general informational purposes only and does not constitute medical advice, diagnosis, or treatment. Thyroid conditions require professional medical evaluation and individualized treatment planning. Always consult a qualified endocrinologist or primary care physician if you suspect a thyroid disorder. Do not discontinue or alter any prescribed medication based on information in this article. The author and publisher accept no liability for actions taken based on this content.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.