Elderly Parent Sleepy and Confused: Hypoactive Delirium or Aging?
An elderly parent who is suddenly sleepy and confused may be experiencing hypoactive delirium, an acute brain failure triggered by underlying medical issues such as UTIs, dehydration, constipation, pain, hypoxia, or medication changes. Unlike normal aging, which develops gradually over years, delirium begins rapidly over hours to days and fluctuates. Immediate medical evaluation is required.

Executive Summary
Sudden sleepiness, quiet withdrawal, and confusion in an older adult should not be dismissed as normal aging. In people aged 60 and above, these changes may indicate hypoactive delirium, a quiet form of acute brain failure that can be triggered by infection, dehydration, medication effects, pain, constipation, hypoxia, or metabolic imbalance.
This guide explains how families and clinicians can distinguish normal fatigue from delirium by focusing on onset, fluctuation, attention, arousal, and reversible medical triggers. It also outlines validated screening tools, urgent red flags, and non-pharmacological care strategies that support recovery and reduce recurrence risk.
Introduction: The Challenge of Unrecognized Acute Brain Failure in Geriatric Care
If you are asking, “Why is my elderly parent sleepy and confused?” or you notice your elderly parent suddenly sleeping a lot and confused, you are likely witnessing more than standard exhaustion. When a senior family member becomes confused at night and sleepy during the day, they may be experiencing a medical crisis known as hypoactive delirium. This presentation of acute cognitive decline, daytime somnolence, and mental confusion is one of the most critical yet frequently misunderstood clinical scenarios in geriatric medicine.
While hyperactive delirium — characterized by agitation, hallucinations, and combative behavior — demands immediate attention due to its disruptive nature, hypoactive delirium is characterized by a silent, hypo-alert state that is easily overlooked. This “quiet” form of brain failure represents an acute neuropsychiatric syndrome driven by underlying organic pathologies that threaten the life of the patient.
Statistically, delirium is a major challenge in acute and long-term care settings. Approximately 30 percent of hospitalized older adults over the age of 65 experience delirium, with rates escalating to 50 percent following major surgery, and up to 80 percent in intensive care units. Among these cases, hypoactive and mixed motor subtypes are the most common presentations in geriatric populations, accounting for up to 80 percent of all delirium diagnoses.
Because the symptoms of hypoactive delirium are subtle — often presenting simply as an older parent appearing unusually quiet, sleepy, or disengaged — the condition remains unrecognized in up to 70 percent of clinical cases. Delayed diagnosis directly correlates with poor patient outcomes, including a higher risk of permanent cognitive decline, accelerated progression of underlying dementia, prolonged hospital stays, premature institutionalization, and significantly elevated short- and long-term mortality rates.
Differentiating between healthy aging and acute neuropsychiatric syndromes is crucial for initiating the rapid diagnostic and non-pharmacological interventions needed to reverse acute brain failure and promote long-term cognitive recovery.
Is Your Elderly Parent Sleepy and Confused? Delirium vs. Dementia vs. Aging
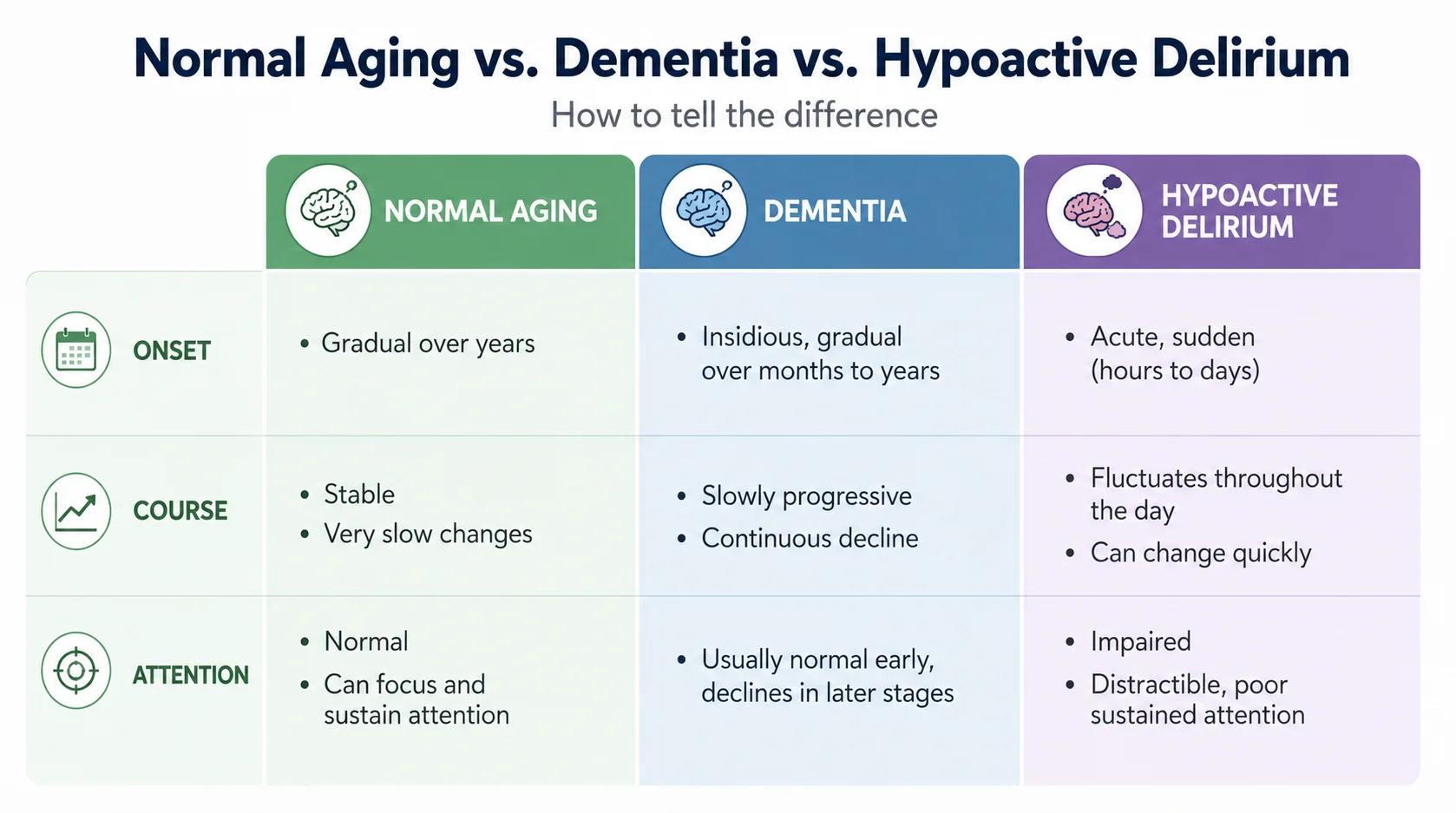
Differentiating between healthy senescence, progressive neurodegenerative disease, and acute neuropsychiatric syndromes requires a structured diagnostic approach. Healthy senescence is characterized by a gradual, predictable decline in physiological reserve. While older adults may experience mild alterations in sleep-wake architecture, such as advanced sleep phase syndrome, their baseline cognitive orientation, executive functioning, and ability to maintain focused attention remain intact during waking hours.
In contrast, dementia is a chronic, progressive primary neurocognitive disorder that develops slowly over months to years. While individuals with advanced dementia exhibit significant cognitive deficits, their mental status is consistent from day to day, and their level of arousal is typically unaffected until the terminal stages of the disease.
Hypoactive delirium represents a sudden and fluctuating departure from an individual’s cognitive baseline. Its onset occurs rapidly, unfolding over a period of hours to days, and is defined by a fluctuating clinical course throughout the day. An older adult experiencing hypoactive delirium may appear lucid and responsive during morning hours but become profoundly somnolent, distracted, and disoriented by the afternoon.
The defining diagnostic feature that distinguishes hypoactive delirium from both healthy aging and dementia is a profound impairment in attention and environmental awareness.
| Clinical Dimension | Healthy Senescence (Aging) | Dementia (Chronic Neurodegeneration) | Hypoactive Delirium (Acute Brain Failure) |
|---|---|---|---|
| Onset Profile | Gradual, tracking over years. | Slow and progressive over months to years. | Acute, developing over hours to days. |
| Cognitive Trajectory | Stable, showing no acute fluctuations. | Steady, progressive slow decline. | Highly fluctuating; symptoms wax and wane. |
| Attention & Concentration | Preserved; normal concentration. | Generally intact in mild-to-moderate stages. | Severely impaired; inability to focus or shift attention. |
| Level of Arousal | Normal; daytime alertness is preserved. | Alert and awake during the daytime. | Altered; marked somnolence, lethargy, or stupor. |
| Reversibility Potential | Permanent biological process. | Irreversible, progressive neurodegeneration. | Highly reversible upon treating underlying causes. |
| Psychomotor State | Normal; age-appropriate mobility. | Typically normal until late stages. | Retarded; hypo-alert, withdrawn, quiet. |
| Sleep-Wake Cycle | Slightly advanced; normal structure. | Relatively stable; some nighttime waking. | Severely disrupted; daytime sleepiness with night waking. |
| Speech and Language | Intact; minor word-finding pauses. | Aphasic; progressive word-finding difficulties. | Slow, incoherent, rambling, or completely absent. |
Neurobiological Pathways: The Pathophysiology of Hypoactive Delirium
The vulnerability of the aging brain to acute cognitive dysfunction is rooted in a progressive decline of physiological reserve, a concept known as reduced cerebral reserve. As the brain ages, it undergoes structural and metabolic shifts, including subclinical microvascular changes, neuronal loss, and a decrease in cerebral perfusion. These changes compromise the brain’s ability to maintain homeostatic stability under acute physiological stress.
When an acute stressor occurs, it triggers a cascade of neurobiological pathways that culminate in hypoactive delirium. This process involves several primary mechanisms:
Neuroinflammation and Blood-Brain Barrier Disruption
Systemic inflammatory insults — such as infections, major surgeries, or tissue trauma — induce the release of peripheral pro-inflammatory cytokines (including tumor necrosis factor-alpha [TNF-α], interleukin-1 [IL-1], and interleukin-6 [IL-6]). In vulnerable older adults, these peripheral cytokines compromise the endothelial cell-cell tight junctions of the blood-brain barrier. This increased permeability allows inflammatory mediators to enter the central nervous system, activating microglia and astrocytes. The resulting neuroinflammatory response causes localized ischemia, synaptic dysfunction, and transient neuronal damage.
Neurotransmitter Imbalance
Proper cognitive function relies on the precise balance of various neurotransmitter pathways. Hypoactive delirium is closely tied to a marked reduction in cholinergic activity alongside a relative increase in dopaminergic and noradrenergic transmission. Acetylcholine is the principal neurotransmitter responsible for attention, arousal, and memory consolidation. Under conditions of physiological stress or neuroinflammation, cholinergic synthesis falls, while dopamine levels rise. A decrease in this cholinergic-to-dopaminergic balance impairs the brain’s ability to filter sensory inputs and maintain executive focus, leading to the clinical presentation of confusion and somnolence.
Oxidative Stress and Cellular Injury
The central nervous system is highly susceptible to oxidative damage due to its high oxygen demand, lipid-rich composition, and relatively low antioxidant defenses. Systemic stressors elevate the production of reactive oxygen species (ROS) and reactive nitrogen species (RNS) within the brain. This oxidative stress disrupts mitochondrial function, impairs adenosine triphosphate (ATP) synthesis, and compromises neuronal signaling pathways.
Circadian Rhythm and Melatonin Dysregulation
Disruption of the sleep-wake cycle is a key feature of hypoactive delirium. Physiological stress impairs the normal secretory patterns of melatonin from the pineal gland, disrupting core body temperature regulation, metabolic processes, and immune defenses. This dysregulation leads to daytime sleepiness and nighttime wakefulness, which further exhausts the brain’s limited cognitive reserve.
Neuroendocrine Stress Responses
Acute illness triggers the hypothalamic-pituitary-adrenal (HPA) axis, causing a sustained release of glucocorticoids. Elevated cortisol levels damage hippocampal neurons, downregulate neurotrophic factors, and increase the brain’s vulnerability to subsequent ischemic or inflammatory damage.
Screening and Diagnosis: Validated Clinical Instruments

Because hypoactive delirium lacks the obvious behavioral disruptions of its hyperactive counterpart — such as agitation, combative behavior, or vocal distress — it is missed in up to 70 percent of clinical cases. Older adults with this condition are often described as “unusually cooperative,” “quiet,” or “just resting.” To prevent this diagnostic gap, clinicians and caregivers must use validated screening tools that focus on objective measures of alertness and attention.
The 4 A’s Test (4AT)
The 4AT is a highly sensitive (88–90%) and specific (92–97%) screening tool designed for rapid clinical evaluation. It is particularly effective because it requires no specialized training and can be completed in under two minutes. Crucially, the 4AT allows for the assessment of severely drowsy or non-verbal patients by assigning specific scores to “untestable” cognitive responses.
- Alertness: The clinician observes the patient’s level of arousal and interaction during the assessment. Fully alert behavior scores 0, mild sleepiness for less than 10 seconds after waking scores 0, and clearly abnormal drowsiness or agitation scores 4.
- AMT4 (Abbreviated Mental Test – 4): The patient is asked to state their age, date of birth, current location, and current year. Zero mistakes score 0, one mistake scores 1, and two or more mistakes or an untestable state score 2.
- Attention (Months Backwards): The patient is asked to recite the months of the year backward from December. Successfully reciting seven or more months scores 0, starting but scoring fewer than seven months scores 1, and being untestable due to drowsiness or inattention scores 2.
- Acute Change or Fluctuating Course: The clinician determines if there is evidence of a rapid deterioration in mental status arising over the last two weeks and still evident in the last 24 hours. No change scores 0, and a documented acute change scores 4.
A total score of 4 or more indicates likely delirium and warrants an immediate, thorough medical review. A score of 1 to 3 suggests potential chronic cognitive impairment, requiring further formal diagnostic workup.
The Confusion Assessment Method (CAM)
The Confusion Assessment Method (CAM) remains the clinical gold standard for diagnosing delirium. Unlike screening scores, the CAM relies on a specific diagnostic algorithm based on four primary features:
- Acute Onset and Fluctuating Course: Evidence of a sudden change in mental status from baseline, with symptoms that tend to wax and wane during the day.
- Inattention: Difficulty focusing, maintaining, or shifting attention, often observed during a brief conversation.
- Disorganized Thinking: Ramshackle, illogical, or incoherent flow of ideas, characterized by rambling speech or unpredictable topic switching.
- Altered Level of Consciousness: Any state of arousal other than “alert” (e.g., vigilant, lethargic, stuporous).
A positive diagnosis of delirium requires the presence of both Feature 1 and Feature 2, along with either Feature 3 or Feature 4. To measure symptom intensity over time, clinicians use the Confusion Assessment Method-Severity (CAM-S) score. The CAM-S Short Form uses a scale of 0 to 7, while the Long Form ranges from 0 to 19, with higher scores strongly tied to adverse outcomes like increased mortality and longer hospital stays.
Hypoactive Delirium Validation Studies in Palliative Populations
Clinical settings like oncology and palliative care units present unique diagnostic challenges due to overlapping symptoms of end-of-life fatigue, medication side effects, and cognitive decline. Validation research supports using structured tools in these populations.
| Assessment Instrument | Sensitivity | Specificity | Target Domain & Clinical Utility |
|---|---|---|---|
| 4 A’s Test (4AT) | 0.89 | 0.94 | Rapid bedside screen; does not require specialized training. Highly effective in hospice and acute care. |
| Confusion Assessment Method (CAM) | 0.88 | 1.00 | Diagnostic algorithm; accuracy relies on rater training and formal cognitive interviews. |
| Brief CAM (bCAM) | 0.80 | 0.87 | Brief adaptation of the CAM; designed for rapid assessment in emergency and palliative environments. |
| Memorial Delirium Assessment Scale (MDAS) | 0.97 | 0.95 | 10-item severity scale; highly effective for monitoring symptom severity and diagnostic thresholds. |
| Delirium Rating Scale-Revised-98 (DRS-R-98) | 0.94 | 0.92 | Comprehensive 16-item clinical rating scale; measures both cognitive and non-cognitive domains of delirium. |
Atypical Silent Infection Manifestations Triggering Geriatric Lethargy
Delirium is a multifactorial syndrome that occurs when acute stressors (precipitating factors) overwhelm a vulnerable patient (who possesses predisposing factors). In highly vulnerable older adults — such as those with pre-existing dementia, severe frailty, or sensory deficits — even minor physiological stressors can precipitate a severe episode of hypoactive delirium.
To guide systematic diagnostic evaluations, clinicians rely on two primary etiological frameworks: the “I WATCH DEATH” mnemonic for identifying underlying systemic causes, and the “PINCHME” framework for identifying common, modifiable triggers.
The “I WATCH DEATH” Clinical Etiology Matrix
The “I WATCH DEATH” framework helps identify the systemic and medical causes of acute brain failure. Each component represents a specific pathophysiological stressor that must be systematically investigated through clinical and laboratory evaluations.
| Component | Pathophysiological Mechanism | Clinical & Diagnostic Evaluation |
|---|---|---|
| I – Infection | Systemic inflammatory response and cytokine translocation disrupt blood-brain barrier integrity. | Complete blood count, blood cultures, urinalysis with microscopic examination, chest X-ray. |
| W – Withdrawal | Abrupt reduction in GABAergic tone or cholinergic transmission causes receptor-level instability. | Comprehensive review of prescription and over-the-counter use; assess for benzodiazepine and sedative use. |
| A – Acute Metabolic | Acid-base imbalances, azotemia, and hyperosmolality directly impair neuronal membrane potentials. | Serum electrolytes, renal function panel (BUN, creatinine), liver function tests, serum ammonia. |
| T – Trauma | Systemic tissue trauma, inflammatory pain signaling, and orthopedic injuries trigger autonomic stress. | Visual body inspection, skeletal radiographs, non-contrast head CT scan for suspected intracranial trauma. |
| C – CNS Pathology | Focal or global cerebral ischemia, post-ictal states, or mass effects directly compromise neural networks. | Focused neurological examination, continuous EEG monitoring, brain magnetic resonance imaging. |
| H – Hypoxia | Cellular oxygen starvation impairs oxidative phosphorylation and ATP synthesis in cerebral tissue. | Pulse oximetry, arterial blood gas analysis, electrocardiogram, cardiac troponins, CT pulmonary angiogram. |
| D – Deficiencies | Nutritional depletion of critical cofactors compromises central metabolic pathways and myelin maintenance. | Serum Vitamin B12, red blood cell folate levels, serum thiamine (vitamin B1). Complete nutritional assessment. |
| E – Endocrinopathies | Hormonal imbalances impair central glucose utilization and thyroid-regulated cerebral metabolism. | Rapid capillary glucose, thyroid panel (TSH, Free T4), serum cortisol, serum adrenocorticotropic hormone. |
| A – Acute Vascular | Hypoperfusion from cardiovascular failure or shock leads to generalized cerebral ischemia. | Continuous hemodynamics, central venous pressure, echocardiography, cardiac output monitoring. |
| T – Toxins / Drugs | Exogenous compounds directly cross the blood-brain barrier, causing acute neurochemical disturbances. | Medication reconciliation, toxicology screening, serum drug level monitoring (e.g., digoxin, antiepileptics). |
| H – Heavy Metals | Chronic or subacute heavy metal toxicity leads to progressive neurotoxicity and structural damage. | 24-hour urine heavy metal collection, whole-blood lead, mercury, and arsenic levels. |
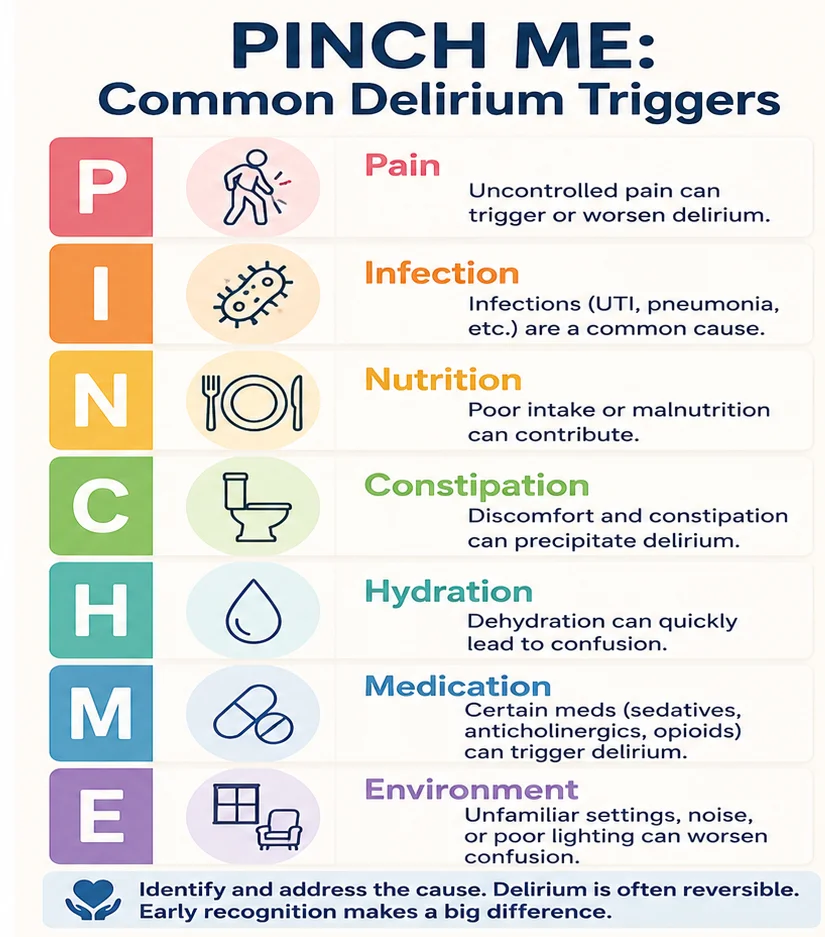
The “PINCHME” Modifiable Trigger Protocol
In daily care, the simpler “PINCHME” framework helps identify and manage the most common, modifiable triggers of hypoactive delirium:
- P – Pain (Pills): Unmanaged pain is a major trigger of cognitive distress. Conversely, over-prescribing highly sedating pain medications (such as opioids) can induce profound daytime somnolence and worsen hypoactive delirium.
- I – Infection (Pus): Infections in older adults frequently present atypically. Rather than a high fever, a silent urinary tract infection or early pneumonia may present solely as daytime lethargy, poor appetite, and sudden confusion.
- N – Nutrition: Acute nutritional deficiencies or rapid shifts in glucose levels can quickly impair brain function.
- C – Constipation (Poo): Severe fecal impaction can cause significant autonomic stress and discomfort, triggering acute confusion in frail older adults.
- H – Hydration (Pee): Dehydration, hypovolemia, and acute urinary retention generate profound physiological stress.
- M – Medication (Pills): Starting high-risk medications (especially those with strong anticholinergic or sedative effects) or sudden drug withdrawals are common precipitating causes.
- E – Environment: Unfamiliar environments, sensory overload, lack of sleep, or sensory deprivation (such as misplacing glasses or hearing aids) severely compromise an older adult’s ability to stay oriented.
Non-Pharmacological Circadian Restoration for Geriatric Lethargy
Large-scale clinical evidence demonstrates that pharmacological agents are not effective for preventing or curing delirium. Antipsychotics (such as haloperidol, risperidone, or olanzapine) should not be used routinely for hypoactive delirium; they are reserved for cases involving severe distress, active hallucinations, or behaviors that pose an immediate safety risk. Instead, the primary strategy for managing and preventing hypoactive delirium relies on multicomponent, non-pharmacological interventions.
The Hospital Elder Life Program (HELP) is an internationally recognized, evidence-based system designed to prevent delirium and preserve cognitive and physical function in older adults. A landmark controlled clinical trial involving 852 hospitalized older adults demonstrated that the HELP strategy reduced the incidence of delirium by 40%. This multicomponent approach also significantly shortened the duration of delirium episodes and decreased overall healthcare costs.
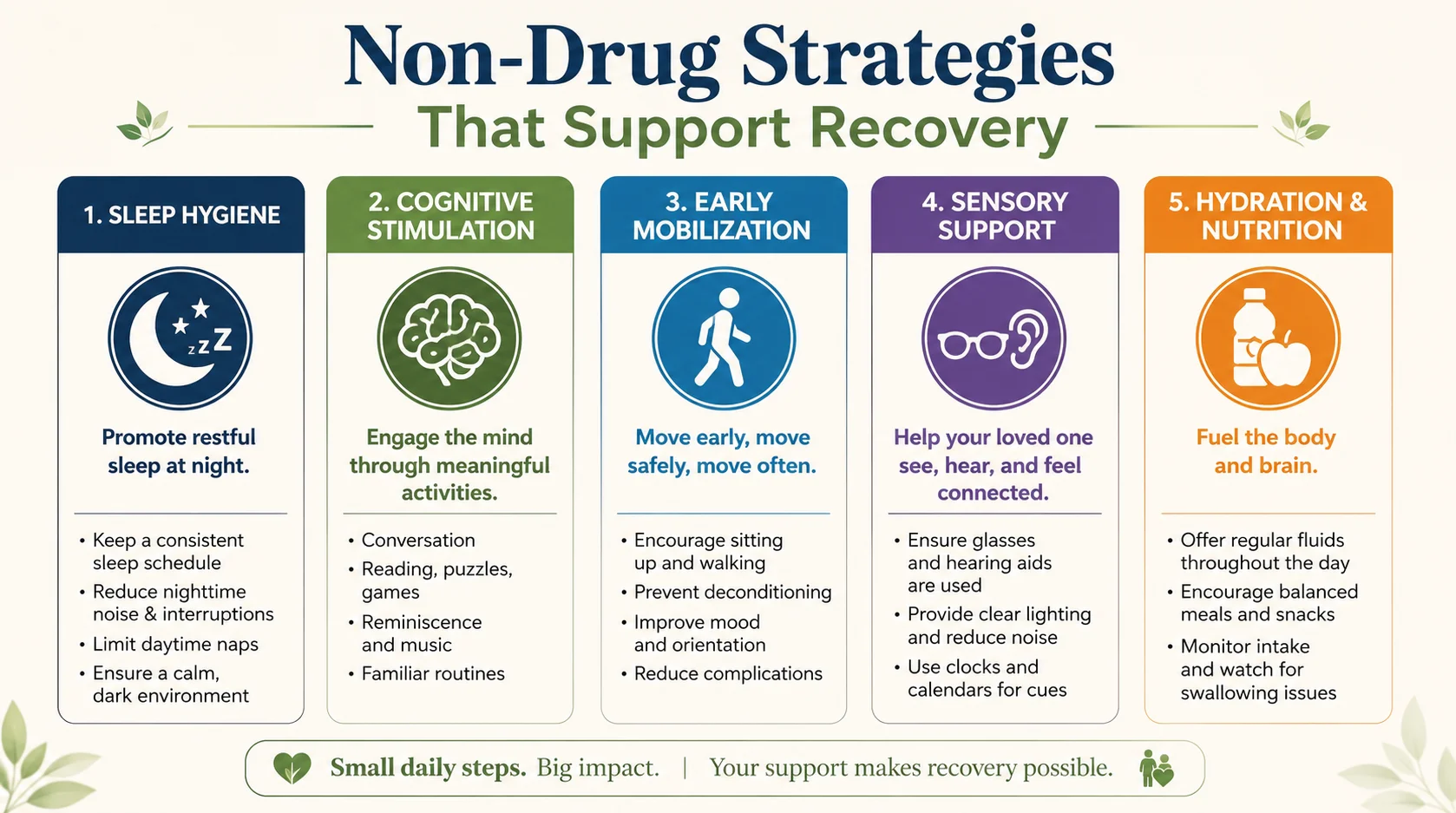
The core interventions of the HELP model address six key risk factors:
Sleep and Circadian Hygiene
To help restore natural circadian rhythms, daytime environments should be brightly lit with natural sunlight, and daytime napping should be discouraged. At night, sleep environments must be kept dark, quiet, and free of unnecessary disturbances. Clinical protocols should group routine medical tasks (such as blood draws and vital sign checks) to avoid waking patients. Instead of prescription sleep medications, sleep is supported using non-pharmacological methods like evening warm drinks, warm milk, gentle back rubs, and relaxing music.
Cognitive Stimulation and Reorientation
Caregivers and clinical staff should frequently reorient the older adult by clearly stating their name, the location, the day of the week, and the plan for the day. Visual aids — such as large-face wall clocks, up-to-date calendars, and orientation whiteboards — should be kept in plain sight. Engaging the older adult in intellectually stimulating, non-stressful activities (such as discussing current events, reading newspapers, reminiscing with family photo albums, or solving simple word puzzles) helps keep brain pathways active.
Early Mobilization and Physical Activity
Prolonged bed rest and physical restraints accelerate cognitive decline and muscle wasting. Older adults should be encouraged to sit out of bed for all meals and walk several times a day when safe to do so. For those unable to walk, passive or active range-of-motion exercises should be performed in bed to maintain circulation and joint mobility.
Vision and Hearing Support
Sensory deprivation can quickly exacerbate confusion and disorientation. Caregivers must ensure that the individual’s prescription eyeglasses and hearing aids are clean, functioning properly, and worn consistently throughout waking hours.
Hydration and Nutritional Maintenance
Dehydration is a strong, independent trigger of acute confusion. Caregivers should offer fluids frequently throughout the day and assist with meals by opening packages, setting up utensils, and ensuring that dentures are properly fitted and worn during meals. Our guide to 10 best foods to eat every day after 60 covers nutrient-dense choices that support this kind of recovery.
Caregiver-Administered Alertness Tracking for Subacute Neurocognitive Shift
Managing an older adult who has been discharged home after a delirium episode, or caring for someone at risk of recurrence, requires structured, everyday protocols. Families can implement these core behaviors using a systematic home-based care plan.
1. Daily Alertness and Cognitive Log
Caregivers should establish a baseline log to track subtle changes in the older adult’s mental state. This log should record daily waking times, daytime sleepiness duration, and basic cognitive responses. Every morning, ask simple orientation questions, such as the current year, season, or day of the week, and note the speed and accuracy of their responses. Any sudden increase in response time or new disorientation should be documented and reported. Chronic pain is a common trigger worth reviewing — see our guide on pain after 60: 6 common types.

2. Environmental and Lighting Adjustments
Reestablishing a clear day-night cycle is critical for biological recovery. During the day, keep blinds and curtains wide open to fill living spaces with natural sunlight. At night, dim the house lights after sunset, turn off televisions and screens, and ensure the bedroom is completely dark and quiet to promote restful sleep.

3. Sensory Aid Audits
Sensory aids help prevent the cognitive isolation that can trigger disorientation. Caregivers should clean eyeglasses and hearing aids daily. Check hearing aid batteries once a week, and confirm that the older adult is wearing both devices as soon as they wake up in the morning. If CPAP-related sleep issues or dry mouth are also part of the picture, see our guide on CPAP dry mouth in older adults.
4. Hydration and Autonomic Protocols
To prevent dehydration and constipation, keep a fresh, clearly labeled water pitcher or bottle near the older adult’s favorite chair. Offer small, frequent glasses of water, diluted juices, or herbal teas throughout the day. Caregivers should also track bowel movements, as constipation can trigger systemic distress and acute confusion in vulnerable older adults.
5. Structured Communication and the TOP5 Model
When interacting with a confused older adult, caregivers can use the TOP5 communication framework:
- Talk to the caregiver: Seek input from family members to understand the patient’s baseline behavior.
- Obtain information: Identify specific, non-verbal signs of distress, pain, or discomfort.
- Personalize care: Tailor conversations and activities to the individual’s lifetime preferences.
- Five strategies: Work with clinical staff to develop five simple, tailored interventions to help calm and orient the individual.
Always speak in short, clear sentences, identify yourself upon entering the room, and use gentle redirection rather than arguing or correcting confused statements.
Home-Based Geriatric Care Cycle
| Morning Protocols | Evening Protocols | Continuous Monitoring |
|---|---|---|
| Open blinds for natural light. | Dim ambient home lighting. | Track hydration and nutrition. |
| Insert clean hearing aids and glasses. | Provide warm, non-caffeinated drinks. | Encourage early mobilization and short walks. |
| Conduct a brief alertness check. | Maintain a dark, quiet sleep space. | Use simple cognitive stimulation games. |

When to Seek Immediate Medical Attention
While home care protocols can support recovery, caregivers must recognize the “red flag” symptoms that require urgent medical evaluation:
- A sudden change in mental status or level of arousal that develops over a few hours.
- Difficulty waking the older adult, or persistent, deep sleepiness.
- Any focal neurological signs, such as slurred speech, sudden facial drooping, or weakness on one side of the body.
- Signs of systemic infection, such as rapid breathing, shortness of breath, or a new, productive cough.
- Complete refusal to eat or drink, or an inability to pass urine for more than 12 hours.
Frequently Asked Questions
The most critical difference lies in the speed of onset and the presence of inattention. Age-related cognitive changes develop gradually over years, and older adults maintain their baseline ability to focus, follow conversations, and remain oriented to time and place. Conversely, hypoactive delirium is an acute syndrome that develops rapidly over hours or days, characterized by a fluctuating level of alertness and a profound inability to focus or sustain attention.
Yes. Pre-existing dementia is the single strongest risk factor for developing delirium. Often, a sudden episode of delirium triggered by a minor illness (such as a UTI or a fall) can “unmask” a mild, underlying dementia that the older adult was previously able to compensate for or hide. Additionally, experiencing an episode of delirium is associated with a higher risk of long-term cognitive decline and future dementia onset.
Hyperactive delirium presents with obvious, hard-to-miss symptoms such as agitation, physical restlessness, hallucinations, and combativeness. Hypoactive delirium presents with the exact opposite: marked sleepiness, quiet withdrawal, slowed movement, and reduced interaction. In busy hospital wards or at home, this quiet behavior is often mistaken for fatigue, depression, or simply “resting quietly,” allowing the underlying medical cause to go untreated.
The most common triggers are summarized by the “PINCHME” framework: unmanaged pain, silent systemic infections (especially urinary tract infections or pneumonia), nutritional deficits, constipation, dehydration, high-risk medications, and sudden environmental changes.
As the immune system ages, older adults often do not mount a typical febrile response or show elevated white blood cell counts during an infection. Instead of classic symptoms like dysuria or fever, the systemic inflammatory response compromises the blood-brain barrier. This triggers a neuroinflammatory cascade that manifests solely as acute brain failure, showing up as sudden daytime sleepiness, confusion, and lethargy.
Delirium is generally considered a reversible condition once the underlying physiological causes (such as infections, metabolic imbalances, or drug toxicities) are resolved. However, while some cases resolve within a few days, recovery can be a slow process in older, frail adults. In about 20% of cases, symptoms can linger for weeks or even months, and some individuals may not fully return to their previous cognitive baseline.
Unlike many cognitive tests that require verbal responses, the 4AT is designed to handle “untestable” situations. If an older adult is too drowsy, lethargic, or inattentive to complete simple cognitive questions or recite the months backward, those sections are scored as “untestable.” This automatically yields a high score, flagging the change as a possible episode of delirium and prompting a medical review.
Using pharmacological sleep aids (such as benzodiazepines, z-drugs, or over-the-counter antihistamines) is highly discouraged. These medications possess strong anticholinergic or sedative properties that can worsen brain failure, prolong the delirium episode, increase the risk of falls, and deepen daytime somnolence. Non-pharmacological sleep support should always be used first.
Many over-the-counter allergy, cold, and sleep medications contain active ingredients (such as diphenhydramine) with strong anticholinergic properties. These drugs block acetylcholine, the key neurotransmitter responsible for attention, arousal, and memory. In older adults with already low cholinergic reserves, this block can quickly trigger severe chemical confusion and somnolence.
The HELP model is an evidence-based, multicomponent care program designed to prevent delirium and functional decline. Its core strategies can be easily adapted for home use. Caregivers can apply these principles by keeping a highly structured daily routine, maximizing natural daytime light, keeping nights dark and quiet, ensuring glasses and hearing aids are worn, offering water frequently, and encouraging daily physical activity.
Prolonged bed rest and immobility increase the risk of physical decline, deep vein thrombosis, pressure injuries, and constipation — all of which generate physiological stress that can prolong delirium. Early mobilization and simple walking help maintain circulation, improve muscle strength, support bowel function, and provide natural sensory cues that keep the brain oriented.
The caregiver should remain calm, use a reassuring tone, and avoid arguing, lecturing, or trying to logically correct the confusion. It is best to validate their feelings (e.g., acknowledging that an experience feels scary) and then gently redirect their attention to a comforting, familiar topic, a photo album, or a relaxing activity.
Dehydration reduces blood volume and impairs electrolyte balance, which is critical for proper neuronal function. In older adults, a reduced sensation of thirst makes them highly vulnerable to dehydration, especially during an illness. This fluid loss can quickly lead to hypernatremia or elevated blood urea nitrogen levels, directly impairing brain function and triggering somnolence and confusion.
Yes. A history of previous delirium is a strong predisposing risk factor. It indicates that the individual has a reduced cognitive reserve and is highly vulnerable to physiological stressors. For these individuals, caregivers should implement non-pharmacological prevention strategies early during any new illness, medical procedure, or change in environment.
An abrupt change in an older adult’s mental status, level of alertness, or ability to focus should always be treated as a medical emergency. Caregivers should seek immediate medical evaluation if the individual is difficult to rouse, shows signs of sudden weakness or slurred speech (suggesting a stroke), displays a high fever, or has gone a full day without eating, drinking, or passing urine.
Conclusion
Distinguishing hypoactive delirium from the natural changes of aging is a critical skill in geriatric medicine and home care. When an older adult suddenly becomes quiet, sleepy, and confused, it should not be dismissed as a normal part of getting older. Instead, it must be recognized as an acute medical event that requires prompt evaluation. By using validated screening tools like the 4AT and implementing structured, non-pharmacological protocols like the HELP model, clinical teams and family caregivers can identify modifiable triggers early. Addressing these underlying issues, maintaining structured circadian routines, and supporting physical mobility can reverse acute brain failure, preserve cognitive function, and help older adults remain independent at home.
This is for informational purposes only. For medical advice or diagnosis, consult a professional.
Authoritative Sources
- Cleveland Clinic – Delirium – Overview of causes, types, and symptoms.
- National Institute on Aging – Cognitive Health and Older Adults – Cognitive risk factors and prevention.
- The 4AT – Rapid bedside delirium screening tool.
- MSD Manual – Delirium – Clinical diagnostic criteria including the CAM.
- MedlinePlus – Delirium – Patient-facing overview of causes and treatment.
- Hospital Elder Life Program (HELP) – Evidence-based delirium prevention model.
- National Institute on Aging – Sleep and Older Adults – Sleep hygiene guidance.
- MedlinePlus – Dehydration – Causes and risks of dehydration in older adults.
- National Institute on Aging – Hearing Loss in Older Adults – Sensory support guidance.
- National Institute on Aging – Aging and Your Eyes – Vision care for older adults.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.