Sudden Confusion and Urine Leakage in an Elderly Parent: Causes and What to Do
When an elderly parent suddenly becomes confused and starts leaking urine at the same time, it is understandably frightening — and it is also a recognizable medical pattern. In older adults, an acute illness or physical problem often shows up first as a change in mental status rather than a clear local symptom. A urinary tract infection, severe constipation, an inability to empty the bladder, dehydration, or a medication side effect can all disrupt brain function enough to cause sudden confusion, known clinically as delirium, while simultaneously causing new urinary leakage.
This guide explains why these two symptoms so often appear together, walks through the most common reversible causes, and outlines the practical next steps for families, including how to access geriatric and home-care support in the United States.
Sudden confusion and new urine leakage in an elderly parent are most often caused by delirium — an acute, reversible disturbance in brain function — triggered by a urinary tract infection, urinary retention, severe constipation, dehydration, or a new medication. Because delirium can disrupt the brain’s normal control over bladder function, both symptoms often appear at the same time. Prompt medical evaluation usually identifies a treatable cause.
Why Do Confusion and Urine Leakage Happen Together?
Maintaining bladder control requires healthy coordination between the bladder muscle, the urethral sphincters, the spinal cord, and inhibitory centers in the brain’s frontal lobe that normally suppress the urge to urinate until it is appropriate. Delirium disrupts this coordination. When an acute illness, infection, or metabolic disturbance affects brain function, the brain’s ability to suppress involuntary bladder contractions can be lost, leading to sudden urinary leakage that was not present before.
According to the National Institute on Aging, urinary incontinence affects roughly 1 in 10 older adults and has many treatable causes. Delirium itself is defined by the NHS inform guide to delirium as an acute, fluctuating disturbance in attention and awareness that develops over hours to days — distinct from the slower decline seen in dementia, though the two can occur together and can be difficult to tell apart without medical evaluation.
In practice, this means sudden confusion and new incontinence are frequently two visible signs of the same underlying problem, rather than two separate issues. Identifying and treating that underlying trigger — most often an infection, constipation, dehydration, urinary retention, or a medication effect — is usually what resolves both symptoms.
The DIAPPERS Framework: Common Reversible Causes of Sudden Incontinence

Geriatricians commonly use the mnemonic DIAPPERS to review reversible causes of new-onset urinary incontinence in older adults. It is a helpful checklist for families and clinicians working through possible causes together.
| Letter | Possible Cause | What It Looks Like |
|---|---|---|
| D | Delirium | Acute confusion disrupts the brain’s normal control over bladder function. |
| I | Infection | A true urinary tract infection can irritate the bladder and, in frail older adults, trigger delirium. |
| A | Atrophic vaginitis | Low estrogen after menopause can thin and irritate the urethral and vaginal tissue. |
| P | Pharmaceuticals | Certain medications impair bladder emptying or cause sedation (see medications section below). |
| P | Psychological | Severe depression or acute distress can reduce motivation or ability to maintain continence. |
| E | Excess urine output | Uncontrolled diabetes or heart failure can increase urine volume beyond what the bladder can manage. |
| R | Restricted mobility | Arthritis, recent illness, or frailty can prevent reaching the bathroom in time. |
| S | Stool impaction | A hard, impacted stool mass can press on the bladder neck and cause overflow leakage. |
Other Common Causes of Sudden Confusion
When evaluating sudden confusion in an older adult, clinicians also look beyond the bladder for other common, reversible triggers, including pain, infection elsewhere in the body (such as pneumonia), poor nutrition or dehydration, constipation, electrolyte imbalances, low blood sugar, thyroid problems, stroke or another new neurological event, new or interacting medications, and disorienting changes in environment such as a hospital stay. A useful practical step for families is to ask a simple question: has the person been noticeably more confused than usual recently? If so, that alone is a strong enough signal to seek prompt medical evaluation.
Is It a Real Infection? Asymptomatic Bacteriuria vs. True UTI
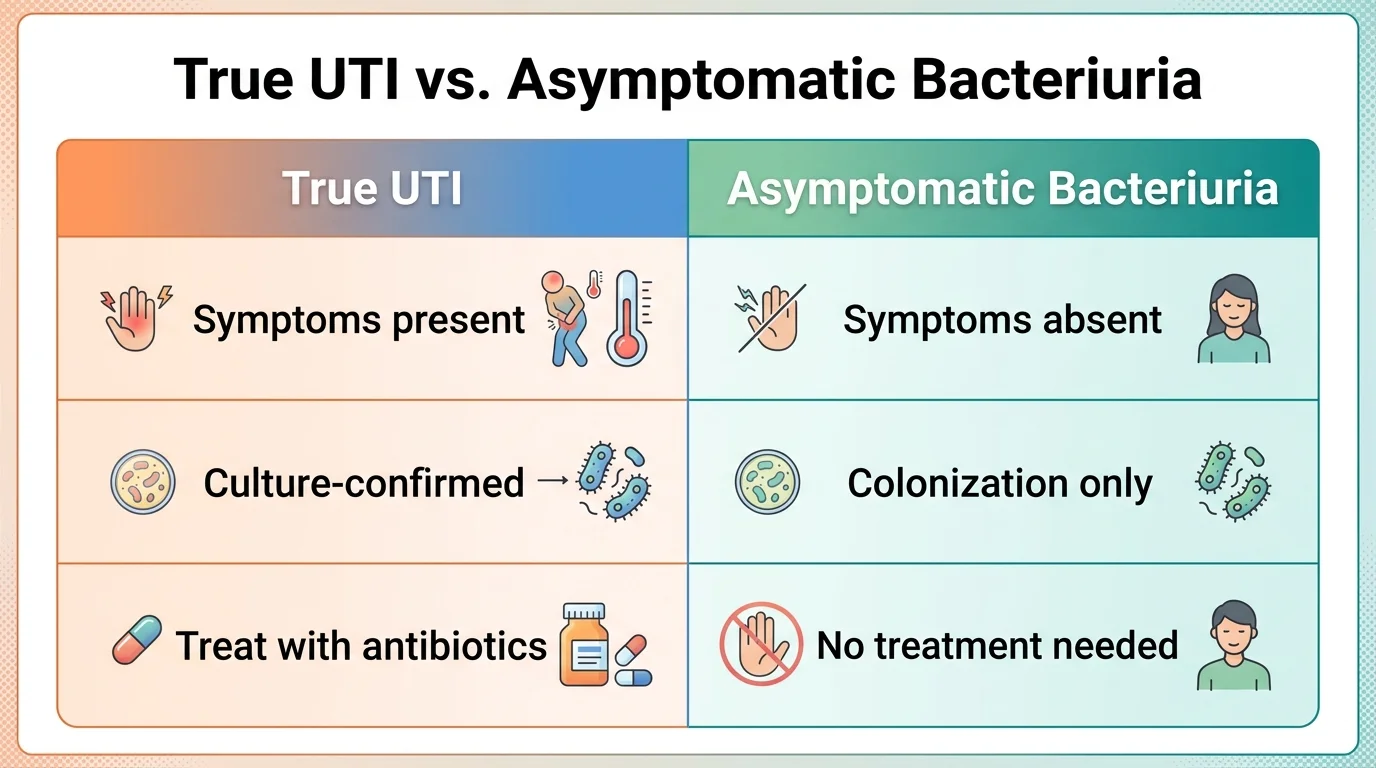
One of the most common diagnostic pitfalls in older adults is assuming that any bacteria found in a urine sample means there is an active infection that needs antibiotics. In reality, many older women — and especially women in their 80s and beyond — have asymptomatic bacteriuria (ASB): bacteria living in the bladder without causing tissue invasion or illness. The Infectious Diseases Society of America’s 2019 guideline and a summary published in American Family Physician both advise against treating ASB with antibiotics, since doing so does not resolve confusion or incontinence and exposes frail patients to unnecessary drug side effects and antibiotic resistance.
A quick urine dipstick test, which checks for leukocytes or nitrites, is frequently positive in older adults simply because of this background colonization — not because of an active infection. Reliable diagnosis of a true UTI generally requires localized symptoms (such as new burning, urgency, or flank pain) alongside a confirmatory urine culture, not a dipstick result alone. If your parent’s confusion or incontinence is blamed solely on “bacteria in the urine” without any of these localized symptoms, it is reasonable to ask the treating clinician whether asymptomatic bacteriuria has been considered before starting antibiotics.
Medications That Can Cause Both Confusion and Urinary Leakage

Certain medications commonly prescribed to older adults can independently cause both cognitive impairment and urinary problems, particularly drugs with anticholinergic or sedating effects. The CDC’s overview of UTIs and the American Geriatrics Society’s Beers Criteria (a widely used list of medications that carry extra risk in older adults) both support reviewing medication lists carefully whenever new confusion or incontinence appears.
| Medication Type | Examples | Why It Matters |
|---|---|---|
| First-generation antihistamines | Diphenhydramine, hydroxyzine | Strongly anticholinergic; can cause drowsiness, confusion, and urinary retention. |
| Overactive bladder medications | Oxybutynin, tolterodine | Cross into the brain easily; can trigger delirium in susceptible older adults. |
| Sedatives / benzodiazepines | Lorazepam, diazepam | Can cause confusion, paradoxical agitation, and increased fall risk. |
| Tricyclic antidepressants | Amitriptyline | Anticholinergic and sedating; can worsen both cognition and bladder emptying. |
If your parent also uses a CPAP machine, medication timing and dry mouth can compound confusion at night — see our guide on CPAP dry mouth in older adults. Never stop a prescribed medication without medical guidance. Instead, bring a full medication list — including over-the-counter drugs and supplements — to the next medical visit and ask specifically whether any of them could be contributing to confusion or urinary problems.
Urinary Retention and Cystocerebral Syndrome
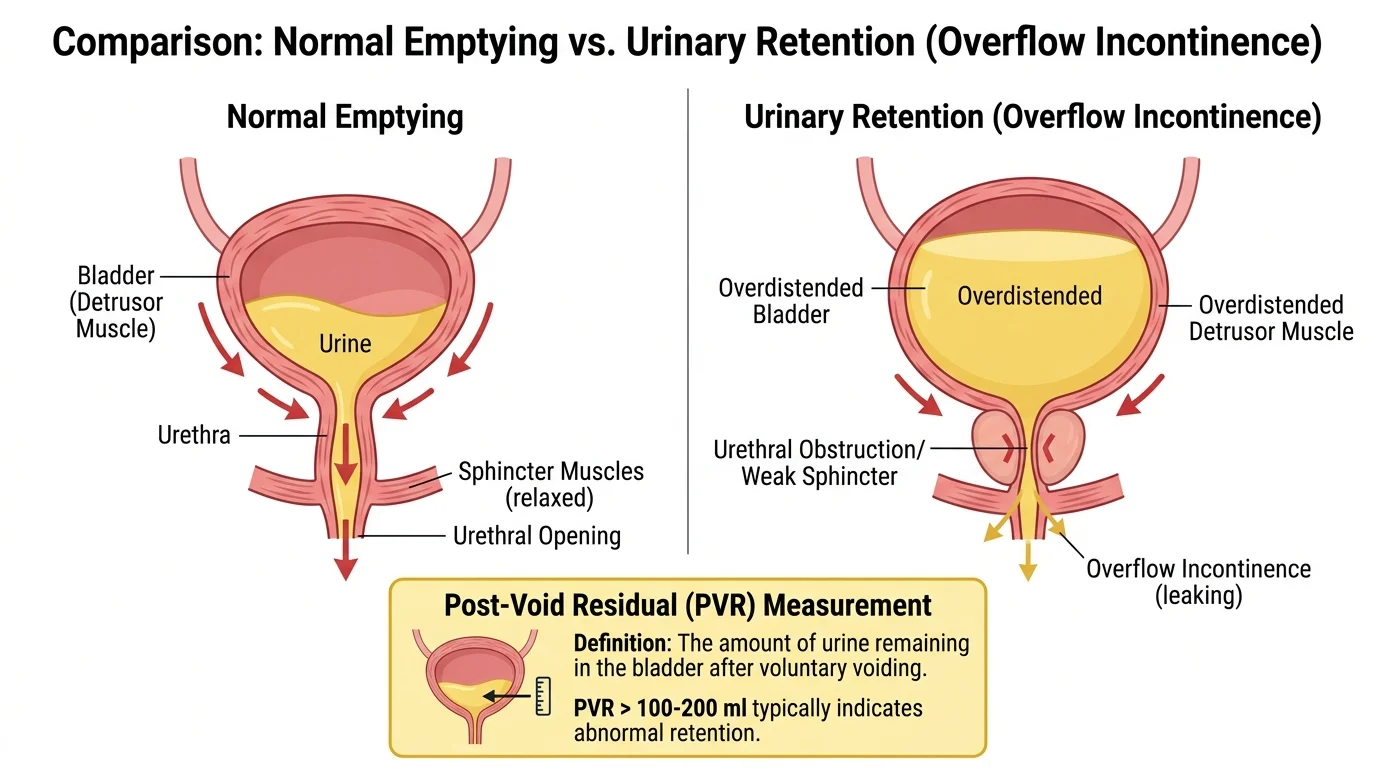
Not all sudden urinary leakage is caused by an overactive bladder. In some cases, the real problem is the opposite: the bladder is not emptying properly, becomes overfilled, and small amounts of urine leak out involuntarily once pressure builds up — a pattern called overflow incontinence. Common causes of urinary retention in older women include severe constipation, pelvic organ prolapse, and anticholinergic medications.
When the bladder becomes significantly overdistended, it can trigger a documented but uncommon phenomenon known as cystocerebral syndrome, in which bladder overdistension itself appears to provoke acute confusion, likely through autonomic nervous system activation. Clinicians typically confirm urinary retention using a simple bedside bladder ultrasound to measure the post-void residual (PVR) volume — the amount of urine left in the bladder after urination. A PVR under 100 mL is generally considered normal, while a PVR of 300 mL or more usually warrants prompt drainage, most often with a temporary catheter, which can rapidly relieve pressure and, in cases of cystocerebral syndrome, resolve the associated confusion.
What to Do: Practical Steps for Families

- Watch for red flags first. High fever, chills, flank pain, inability to urinate at all, low blood pressure, a racing or irregular heartbeat, sudden weakness, or stroke-like symptoms warrant emergency care immediately.
- Confirm whether confusion is truly new. Ask a family member or caregiver who knows the person well whether they have seemed more confused than usual lately — a simple but effective way to flag possible delirium.
- Contact the primary care physician or geriatrician promptly for a non-emergency evaluation, including a medication review, a check for constipation, and a bladder scan if urinary retention is suspected.
- Bring a complete medication list, including over-the-counter drugs and supplements, to the appointment.
- Avoid assuming a urine test alone confirms infection. Ask whether the diagnosis is based on symptoms and a culture, not just a positive dipstick.
Preventing Future Episodes

- Support a nutrient-dense diet, since dehydration and poor nutrition are common contributors to delirium — see our list of 10 best foods to eat every day after 60. Encourage regular fluid intake throughout the day (typically around 1.5 liters unless a clinician has restricted fluids for heart or kidney reasons), reducing intake somewhat in the evening to limit nighttime leakage.
- Set up a scheduled toileting routine, assisting to the bathroom every 2 to 3 hours rather than waiting for the person to ask.
- Address chronic pain safely, since some pain medications carry the same anticholinergic risks discussed above — see our guide on pain after 60: 6 common types. Address constipation proactively with adequate fiber, fluids, and movement, and monitor bowel habits.
- Review medications periodically with a doctor or pharmacist, especially after any new prescription.
- Support orientation by ensuring glasses and hearing aids are worn, keeping the environment familiar and well-lit, and maintaining a consistent sleep-wake routine. The National Institute on Aging’s bladder health tips cover additional practical strategies.
Geriatric and Home-Care Access in the United States

In the US, sudden confusion with new urinary leakage should be treated as a time-sensitive medical presentation. After emergency causes are ruled out, ongoing care is typically coordinated through a primary care physician, geriatrician, or urologist, along with home-based support services depending on insurance status and the level of care needed.
| Resource | What It Offers | How to Access |
|---|---|---|
| Medicare Home Health | Skilled nursing, therapy, and home health aide services for eligible beneficiaries. | Discuss eligibility with the treating physician; see Medicare.gov. |
| Eldercare Locator | Local referrals for transportation, meals, caregiver support, and in-home assistance. | Call 1-800-677-1116 or visit eldercare.acl.gov. |
| Medicaid Home & Community-Based Services | State-run programs supporting personal care and daily living help at home. | Contact your state Medicaid agency or local Aging and Disability Resource Center; eligibility varies by state. |
| PACE (Program of All-Inclusive Care for the Elderly) | Coordinated medical and social services for frail older adults who qualify. | Check CMS PACE resources for local availability. |
| VA Geriatrics and Extended Care | Home-based primary care and long-term care support for eligible Veterans. | Contact the local VA medical center; see VA Geriatrics and Extended Care. |
Frequently Asked Questions
Acute confusion, or delirium, can disrupt the brain’s normal ability to suppress bladder contractions, leading to sudden leakage. She may also have “functional incontinence,” where confusion or mobility limits prevent her from recognizing the urge or reaching the bathroom in time.
No. While UTIs are a common trigger, sudden confusion and incontinence can also result from urinary retention, severe constipation, dehydration, medication side effects, low blood sugar, electrolyte imbalances, or other acute illnesses. A full medical evaluation is needed to identify the actual cause.
Many older women have bacteria present in the bladder without an active infection, known as asymptomatic bacteriuria. Treating this with antibiotics does not improve confusion or incontinence and can expose a frail patient to unnecessary side effects. Diagnosis of a true infection should be based on localized symptoms plus a confirmatory urine culture.
Yes. Medications with anticholinergic or sedating effects, such as some antihistamines, overactive bladder drugs, and benzodiazepines, can impair both brain function and bladder emptying simultaneously. A medication review with a doctor or pharmacist is an important step.
Often, yes. When the underlying cause, such as an infection, urinary retention, or a high-risk medication, is identified and treated promptly, both the confusion and the urinary leakage frequently resolve. Delayed treatment is associated with worse outcomes, so timely evaluation matters.
Cystocerebral syndrome is a documented but uncommon situation where an overfilled, distended bladder itself appears to trigger acute confusion, likely through the autonomic nervous system. It typically resolves quickly once the bladder is drained with a catheter.
Clinicians typically use a bedside bladder ultrasound to measure the post-void residual (PVR) volume, or the amount of urine remaining after urination. A PVR of 300 mL or more usually indicates significant retention requiring prompt drainage.
A large, hard stool mass in the rectum can press against the bladder neck, blocking normal urine flow and causing the bladder to overfill. This leads to small, involuntary leaks known as overflow incontinence, which often improves once the constipation is treated.
Seek emergency care for high fever or chills, flank or back pain, inability to urinate at all, low blood pressure, a fast or irregular heartbeat, sudden weakness, slurred speech, fainting, or any stroke-like symptom.
Families can explore Medicare-covered home health services, the Eldercare Locator for local Area Agency on Aging referrals, state Medicaid Home and Community-Based Services, the PACE program for frail older adults, and VA Geriatrics and Extended Care for eligible Veterans.
Bottom Line
Sudden confusion and new urinary leakage in an elderly parent are almost always signs of an underlying, often treatable problem rather than a permanent decline. The most common triggers are infection, urinary retention, severe constipation, dehydration, or a medication side effect. Getting a prompt medical evaluation — including a careful look at whether any “positive” urine test truly reflects an active infection, and a full medication review — is usually the fastest path back to your parent’s normal baseline.
Authoritative Sources
- National Institute on Aging – Urinary Incontinence in Older Adults – Prevalence, causes, and treatment overview.
- National Institute on Aging – 15 Tips to Keep Your Bladder Healthy – Practical prevention strategies.
- CDC – About Urinary Tract Infections – UTI causes, symptoms, and risk factors.
- NHS inform – Delirium – Delirium definition, causes, and warning signs.
- IDSA – 2019 Asymptomatic Bacteriuria Guideline – Clinical guidance on ASB vs. true UTI.
- American Family Physician – Asymptomatic Bacteriuria – Practical summary for clinicians and families.
- Medicare.gov – Home Health Services – Coverage and eligibility for home health support.
- Eldercare Locator – Local aging-services referrals.
- Medicaid.gov – Home & Community-Based Services – State HCBS program information.
- CMS – Program of All-Inclusive Care for the Elderly (PACE) – Coordinated care for frail older adults.
- VA – Geriatrics and Extended Care – Home-based and long-term care for eligible Veterans.
⚕️ Medical Disclaimer
The information provided on this page is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your diet, starting any supplement, or if you have an existing medical condition. KeepFitQuote does not provide medical diagnoses or treatment recommendations. Read our full disclaimer.